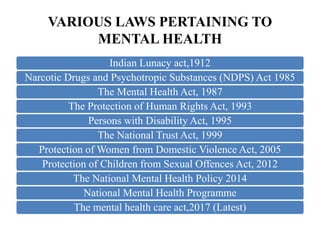
The document discusses India's laws and policies related to mental health, including the evolution from the Indian Lunacy Act of 1912 to the current Mental Healthcare Act of 2017. Some key points:
- The Mental Healthcare Act of 2017 aims to protect the human rights of those with mental illness and fulfill India's obligations under the UN Convention on Rights of Persons with Disabilities.
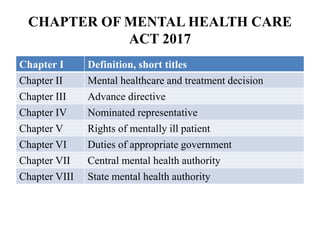
- It decriminalized attempted suicide and introduced concepts such as advance directives, nominated representatives, and rights of persons with mental illness.
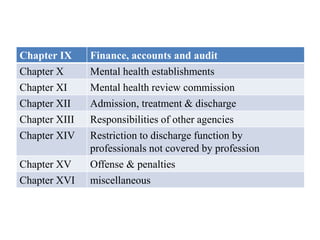
- The act established authorities like the Central Mental Health Authority and State Mental Health Authorities to oversee mental healthcare delivery.
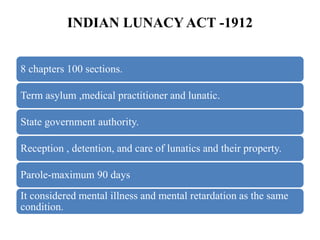
- Compared to previous laws which took a custodial approach, the new