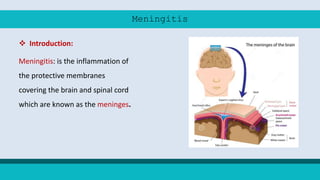
Meningitis is an inflammation of the protective membranes covering the brain and spinal cord. It can be caused by bacteria, viruses, fungi or parasites. Bacterial meningitis caused by Neisseria meningitidis is known as meningococcal meningitis. It commonly affects children under 5 and people over 60. Symptoms include sudden onset of headache, fever, nausea and stiff neck. Prevention includes vaccination, chemoprophylaxis of contacts, and treatment of cases and carriers with antibiotics. Conjugate vaccines provide effective protection against common serogroups.