Download to read offline
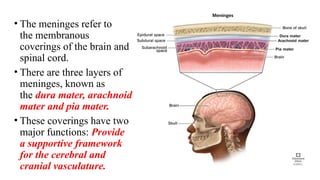
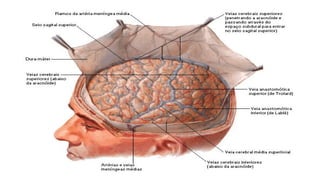
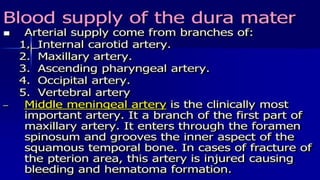
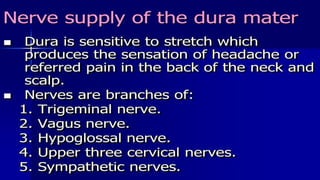
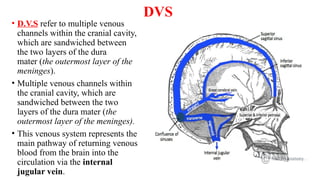
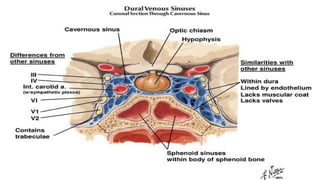
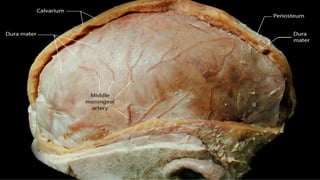
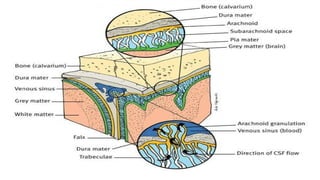
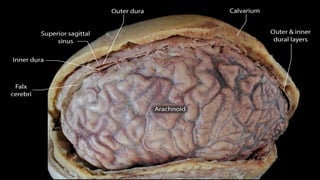
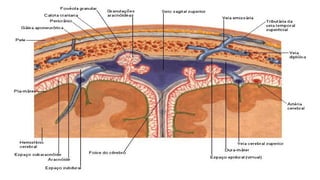
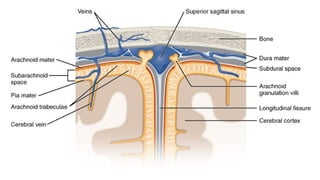
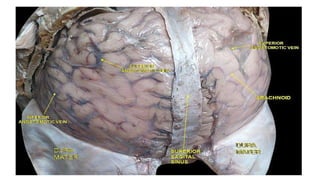
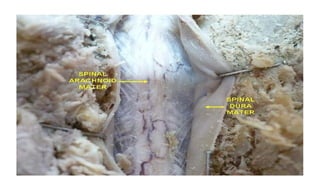
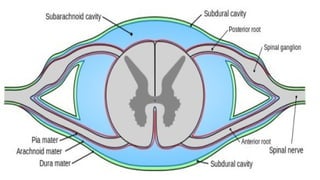
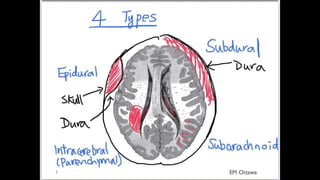
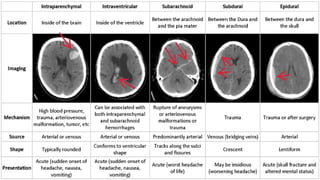
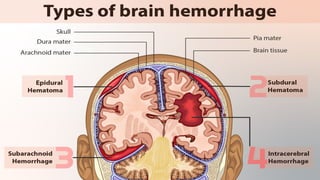
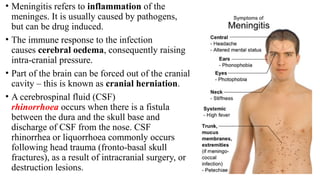

The document provides a detailed overview of the meninges, including their three layers: dura mater, arachnoid mater, and pia mater, along with their functions and structural features. It highlights the differences between cranial and spinal meninges, as well as the clinical significance of various conditions affecting the meninges such as hemorrhages, meningitis, and tumors. Key anatomical details such as dural reflections and venous drainage systems are also discussed.