Downloaded 277 times
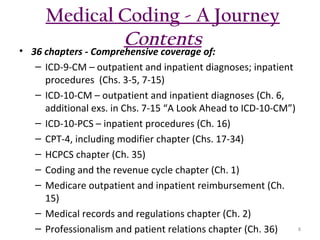





The document outlines the features and rationale behind a medical coding textbook authored by Beth A. Rich, who has extensive experience in healthcare education and management. It aims to engage beginners with practical exercises, real-world scenarios, and accessible language, while equipping instructors with tools to facilitate teaching. Key highlights include 4,673 coding exercises, comprehensive chapters on various coding systems, and additional resources for both students and instructors.




























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






