Download to read offline

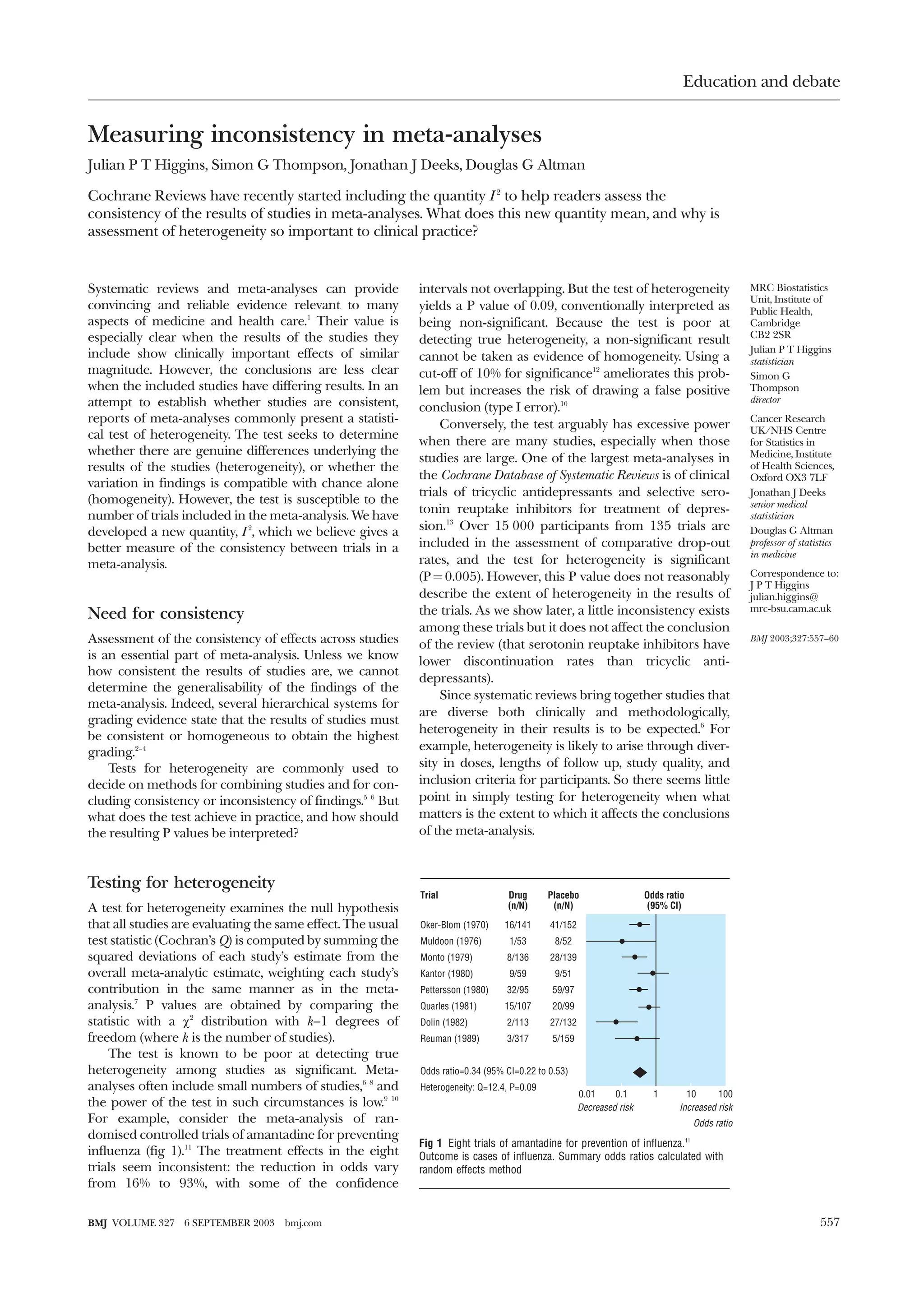




This document discusses a new method for quantifying heterogeneity, or inconsistency, between studies in a meta-analysis called I2. I2 describes the percentage of variation between studies that is due to heterogeneity rather than chance. The document provides examples of I2 values from published meta-analyses to demonstrate its use. I2 can help researchers investigate the causes of heterogeneity by comparing values between subgroups of studies. Quantifying inconsistency with I2 provides a better assessment than significance tests, which are often underpowered and do not measure the size of heterogeneity effects.


































![5ht grade workshop( reading,_writing)[1][1]](https://cdn.slidesharecdn.com/ss_thumbnails/5htgradeworkshopreadingwriting11-110809105543-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)













































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








