Downloaded 38 times

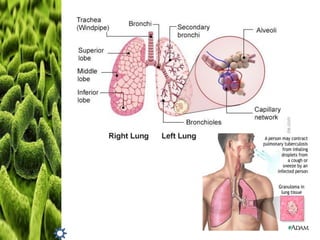


This case study discusses a 52-year-old former tricycle driver diagnosed with multi-drug resistant tuberculosis (MDR-TB) and gout. Prior to admission, the patient experienced fever, severe cough, night sweats, and difficulty breathing. The patient's BMI was normal but he needed to gain weight. The plan was to lower his uric acid levels through diet and exercise to reduce gout risk, gain weight, and follow directly observed therapy to eliminate MDR-TB. The intervention included nutrition counseling, follow up appointments, and lifestyle changes. Evaluation involved reassessing the patient's status and monitoring compliance.