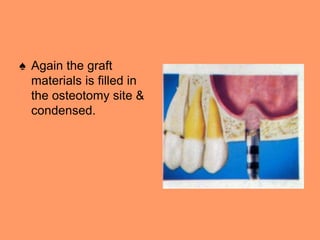
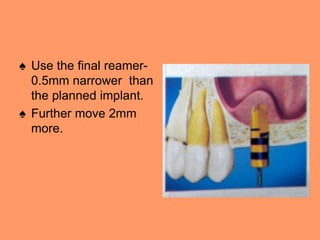
This document provides an overview of the maxillary sinus and sinus lift procedure. It discusses the anatomy of the maxillary sinus, including its dimensions and walls. It then describes the sinus lift procedure, which increases bone mass below the sinus floor to allow for dental implant placement. Several techniques for performing a sinus lift are outlined, including the lateral window approach, osteotome approach, and hatch-reamer system. Pre-operative medications, follow-up considerations, potential complications, and contraindications are also summarized. Diagrams and images are included to illustrate the different approaches.





























































![maxillarysinus-170705134531 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/maxillarysinus-170705134531autosaved-240606120847-09cc00a0-thumbnail.jpg?width=640&height=640&fit=bounds)
![MAXILLARY SINUS AND ITS SURGICAL ANATOMY (2) (1) [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/maxillarysinusanditssurgicalanatomy21autosaved-240927151609-5597be7b-thumbnail.jpg?width=640&height=640&fit=bounds)






















