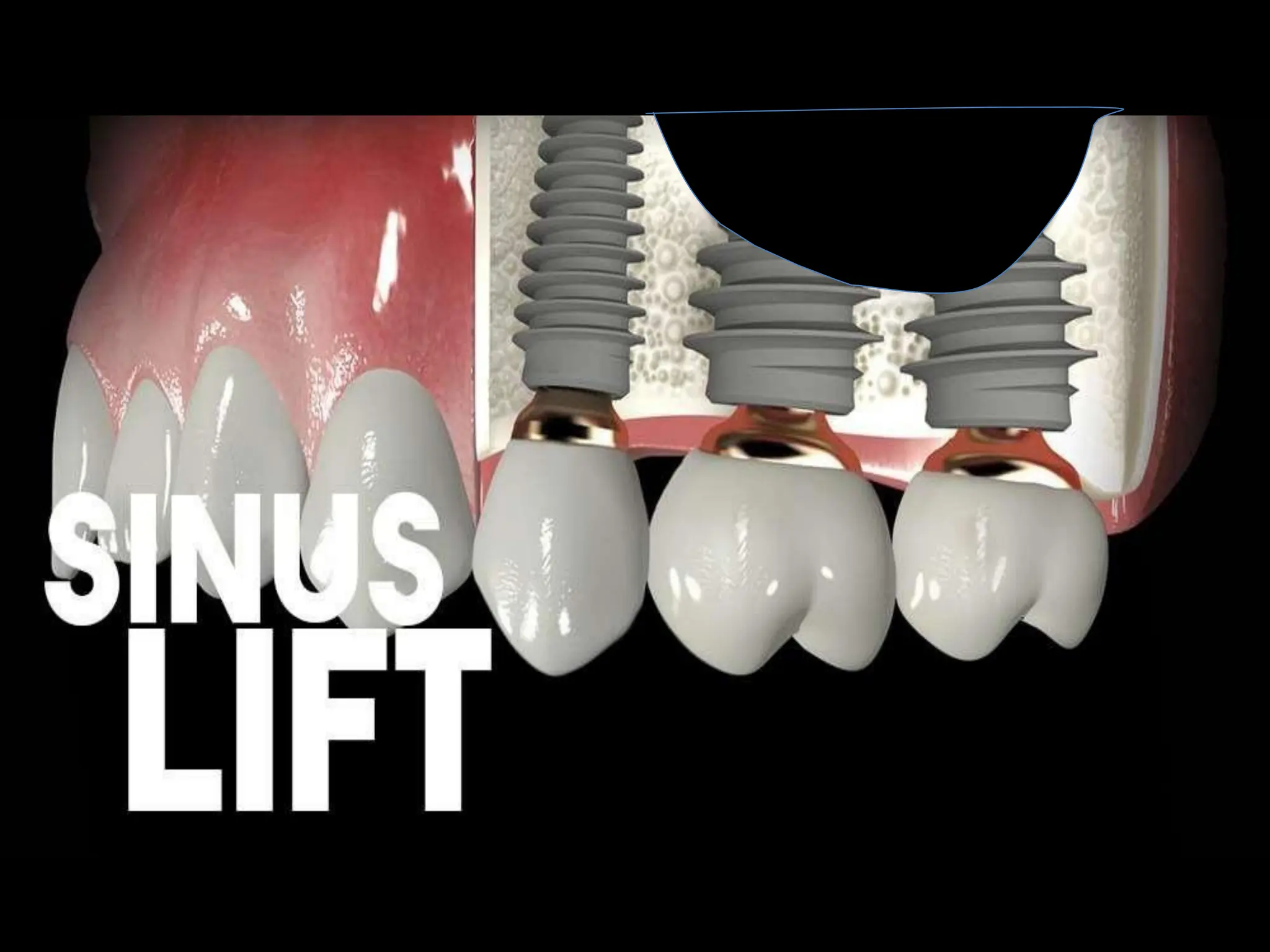
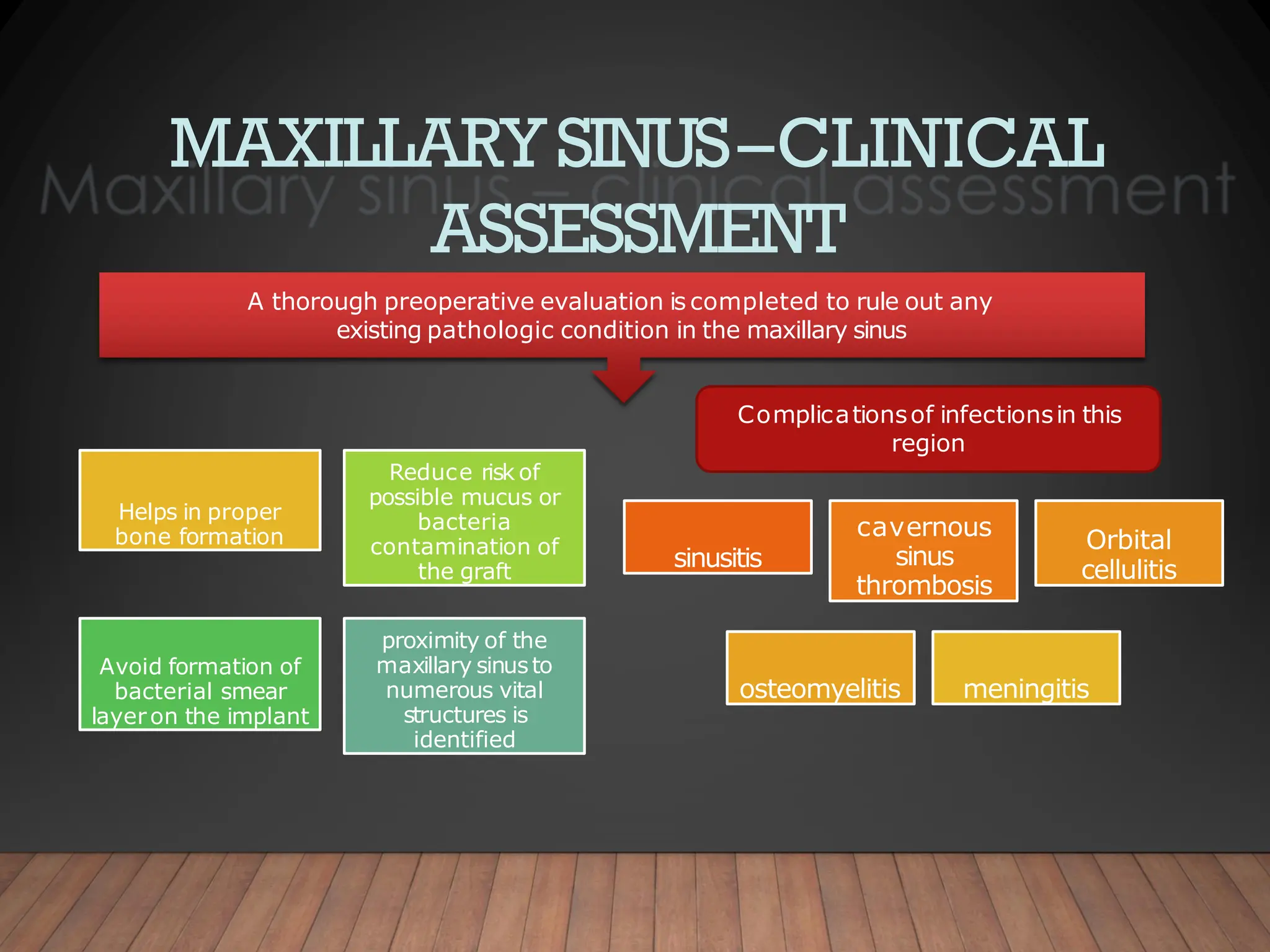
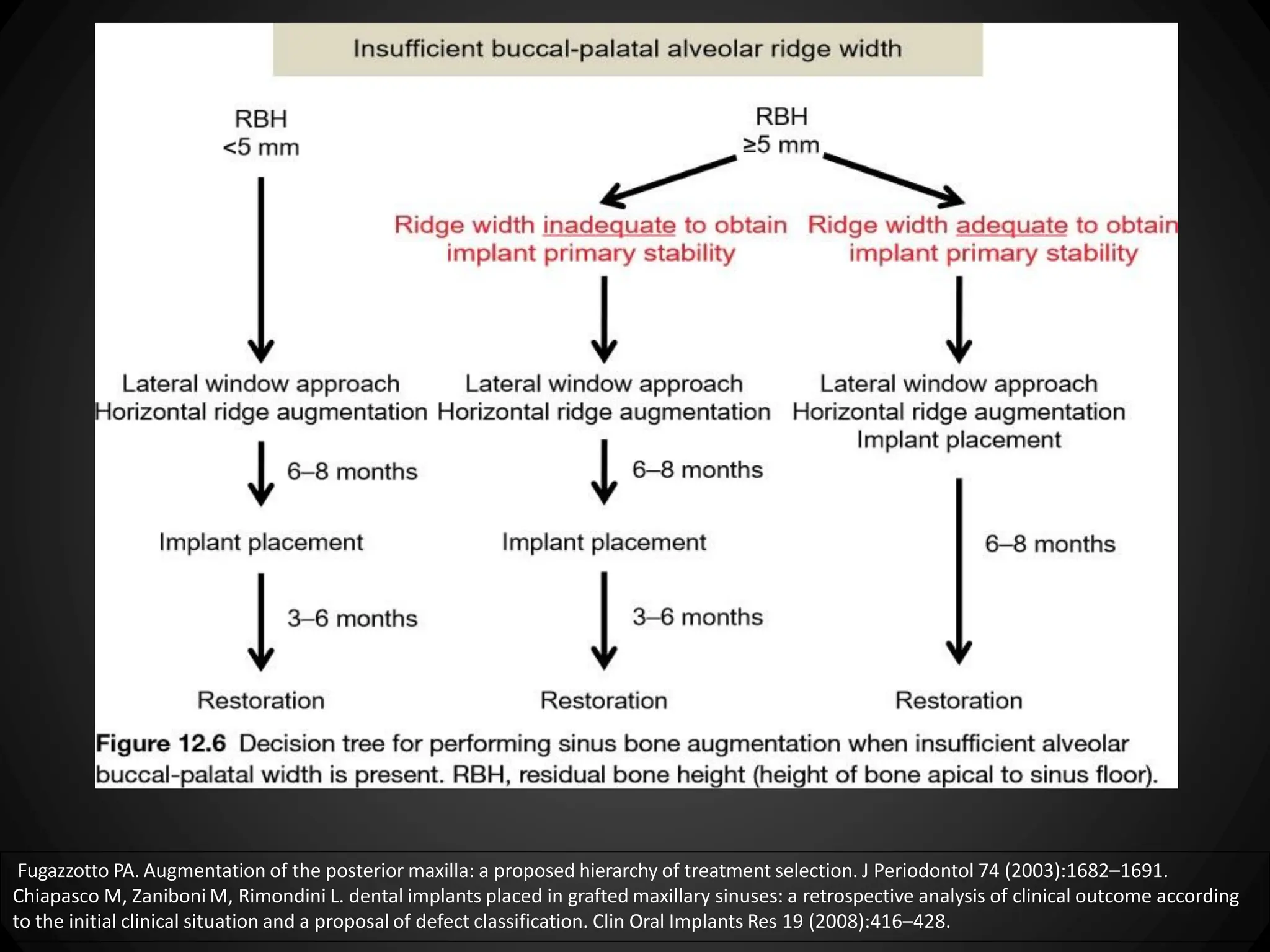
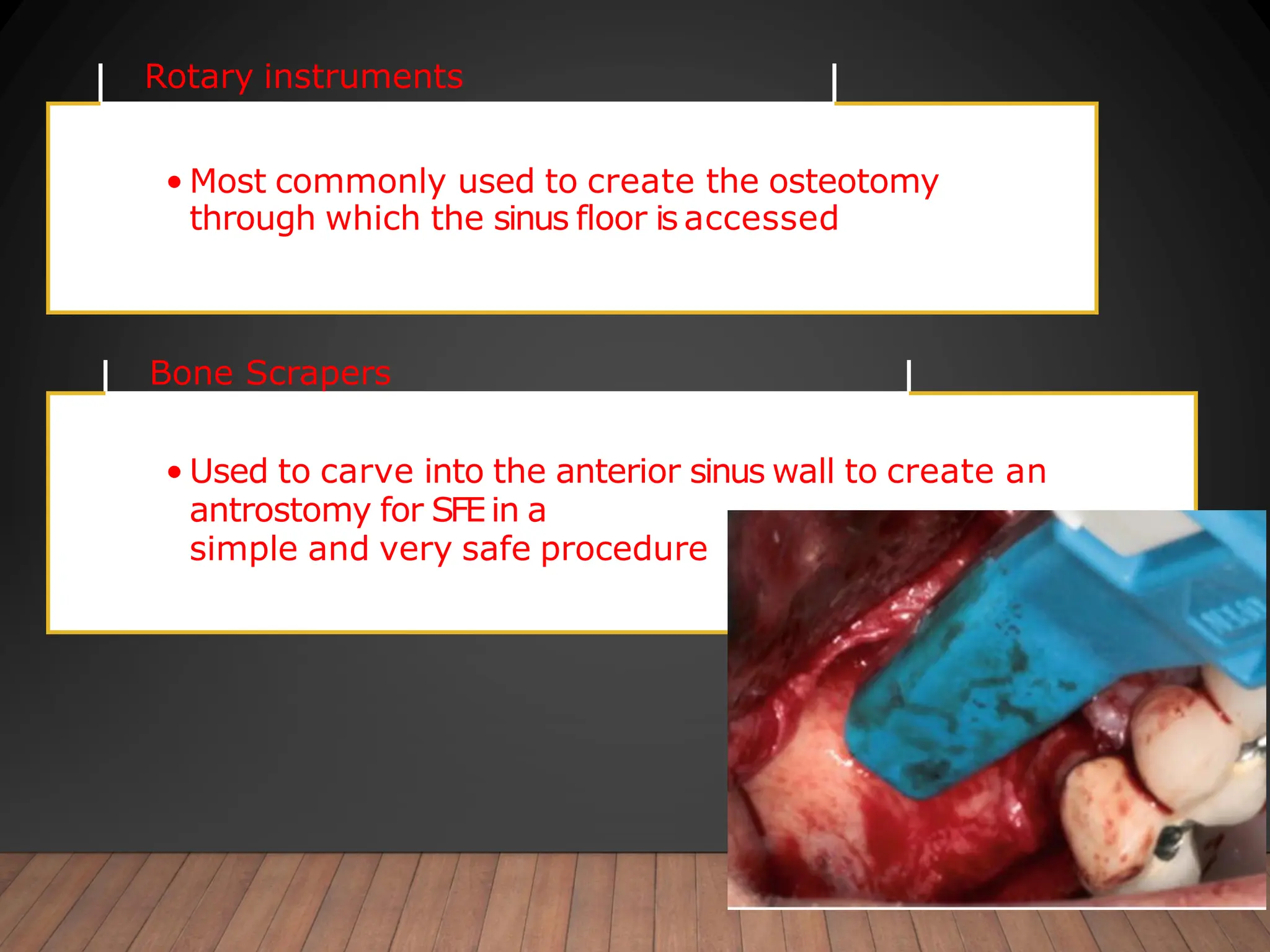
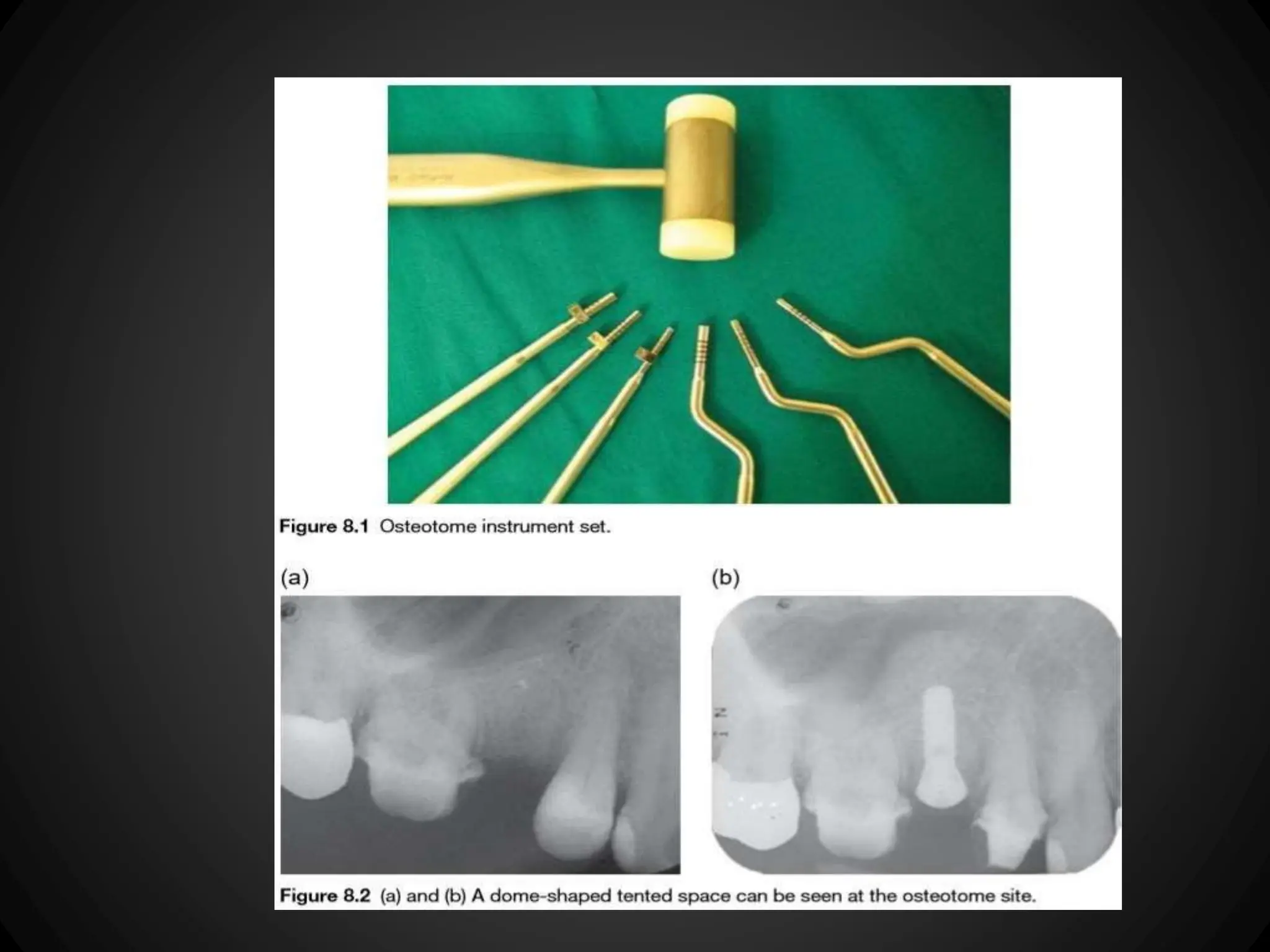
This document discusses the anatomy and surgical procedures related to maxillary sinus lifts. It begins with an introduction describing how maxillary sinus lifts can enable dental implant placement in atrophic maxilla. It then defines the maxillary sinus and describes its anatomy, development, blood supply, nerve supply and functions. It discusses the Schneiderian membrane lining the sinus and various assessment techniques. It provides details on the lateral window and crestal/osteotome approaches to maxillary sinus lifts, including flap design, bone window preparation, membrane elevation, grafting and implant placement. Piezoelectric and Dentium Advanced Sinus Kit techniques are also summarized.














![METHODS OF EXAMINATION
OFTHE INFECTED MAXILLARY
SINUS
CBCT TRANSILLUMINATION NASOENDOSCOPY
MAGNETIC
RESONANCE
IMAGING [MRI]
NASOENDOSCOPY BACTERIOLOGY
CYTOLOGY
FIBREOPTIC
ANTROSCOPY
RADIOGRAPHY
best option
1.Water’s
projection
2.Panoramic
3.Peri apical
Differentiation
of soft tissues
within the
sinus](https://image.slidesharecdn.com/sinusliftppt-240304070925-07523e00/75/Sinus-Lift-ppt-about-maxillary-sinus-lift-28-2048.jpg)



































































































![sinuslift-170526161805.pptxcgfgyuiopkljnmkl;']\](https://cdn.slidesharecdn.com/ss_thumbnails/sinuslift-170526161805-251205045410-d67ed8f9-thumbnail.jpg?width=640&height=640&fit=bounds)


![MAXILLARY SINUS AND ITS SURGICAL ANATOMY (2) (1) [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/maxillarysinusanditssurgicalanatomy21autosaved-240927151609-5597be7b-thumbnail.jpg?width=640&height=640&fit=bounds)



























