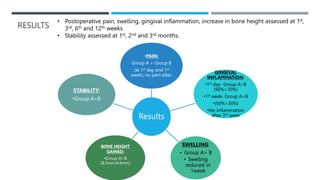
This journal club presentation summarizes a study comparing two techniques for maxillary sinus augmentation: direct sinus lift through a lateral window (Group A) and indirect sinus lift through a crestal approach (Group B). Outcomes were evaluated for pain, swelling, inflammation, bone height gain, and implant stability. For both techniques, pain and swelling reduced after the first week, while inflammation resolved after 3 weeks. Group A saw greater bone height gain (8.5mm vs 4.4mm) but similar stability outcomes. The techniques were deemed successful in allowing for implant placement with augmented sinus bone.


![ Similar findings were observed by Kent and Block [1989], who evaluated clinical outcomes of dental implant
placement and sinus floor elevation and observed that there was no significant pain aft er sinus lift surgery
post operatively
Wiltfang et al observed pain reduction aft er sinus lift surgery with time but found 2 patients with sinusitis
related pain which they found to be due to migration of cancellous bone sequestra into maxillary sinus for
which they performed sinuscopy and removal of sequestrum. Our study correlates to their study in having
minimal pain post surgery](https://image.slidesharecdn.com/journalclubpresentation6-231104095647-0e1fab75/85/JOURNAL-CLUB-PRESENTATION-6-pptx-21-320.jpg)









































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)





