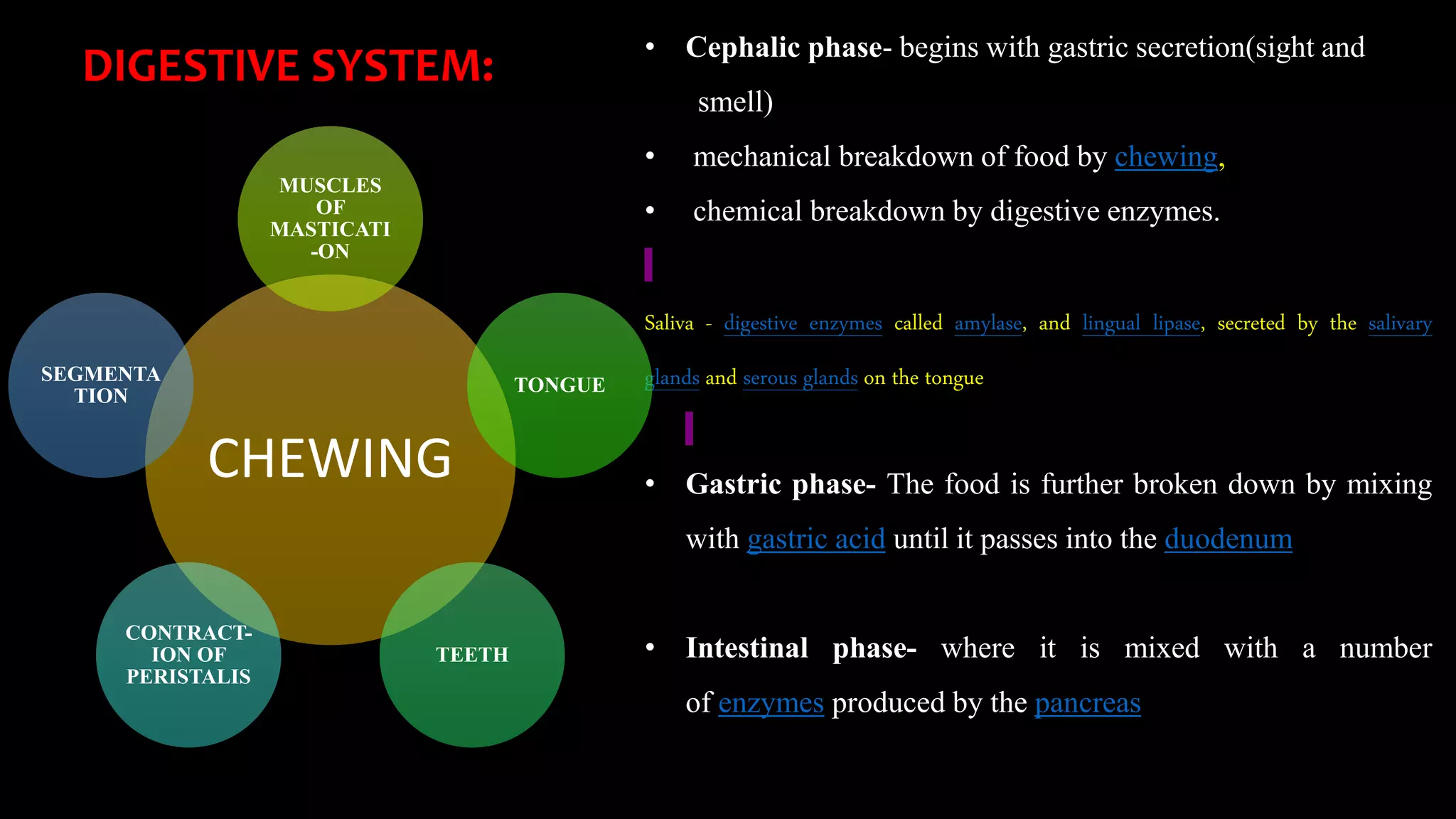
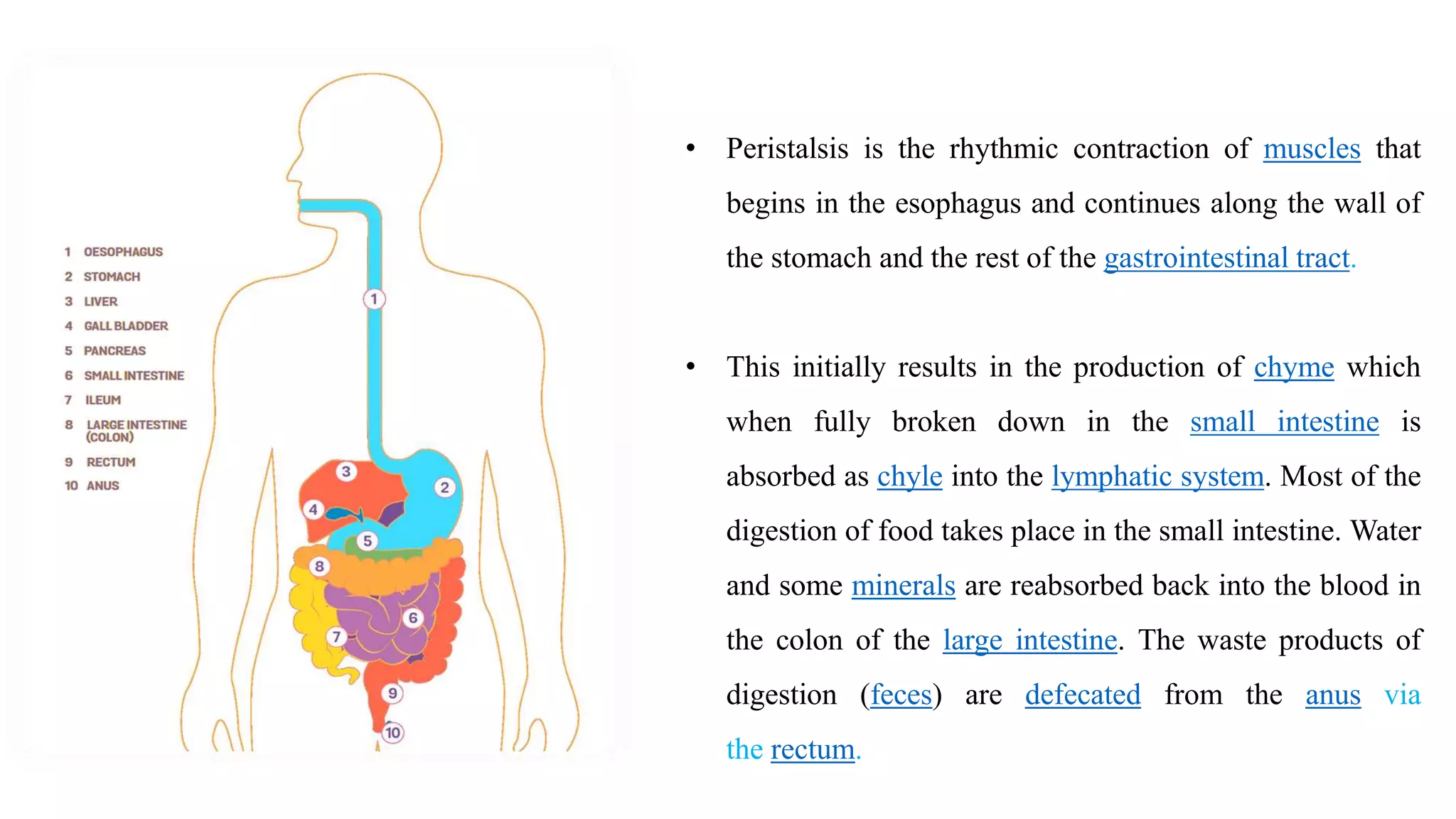
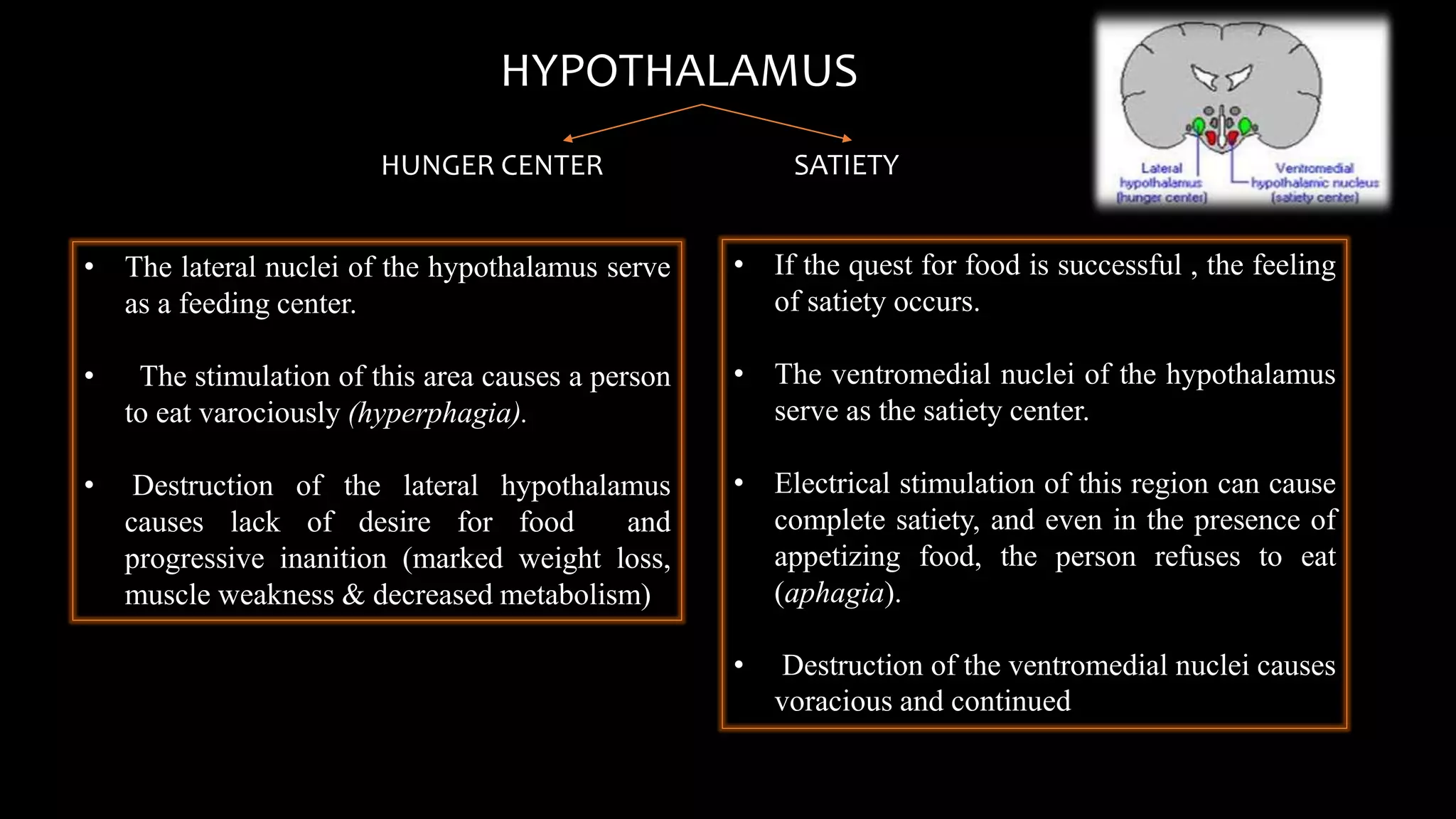
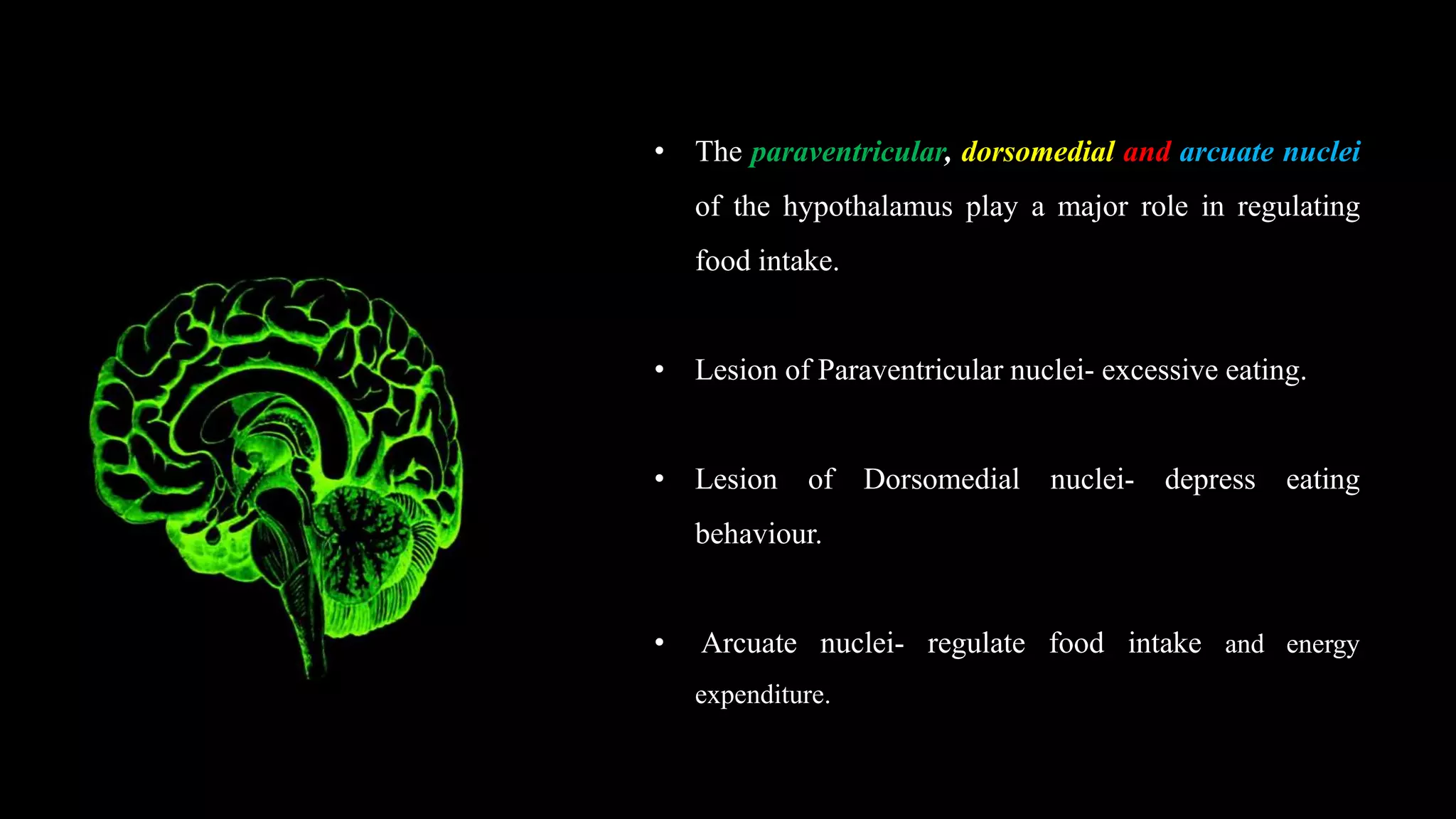
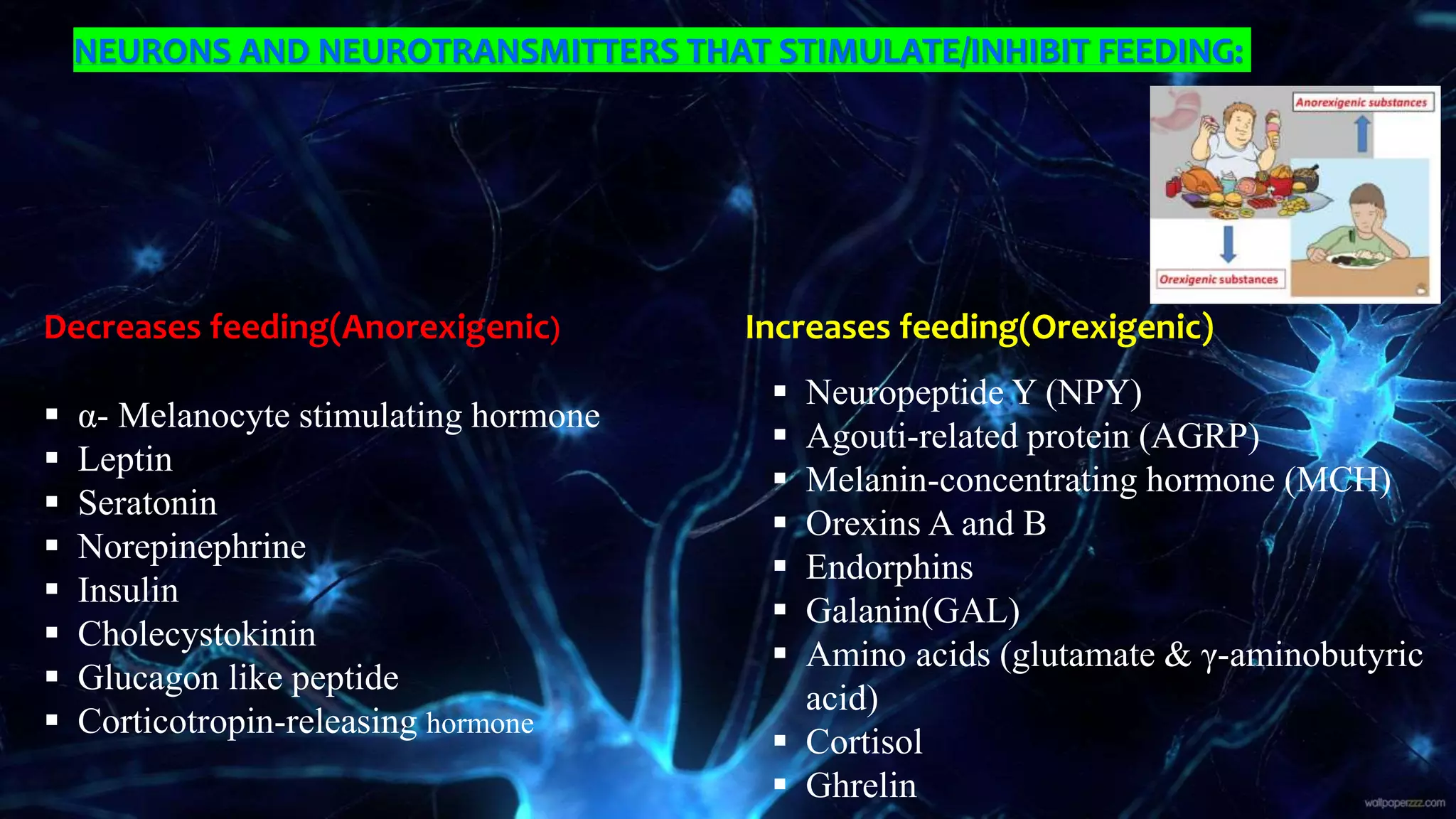
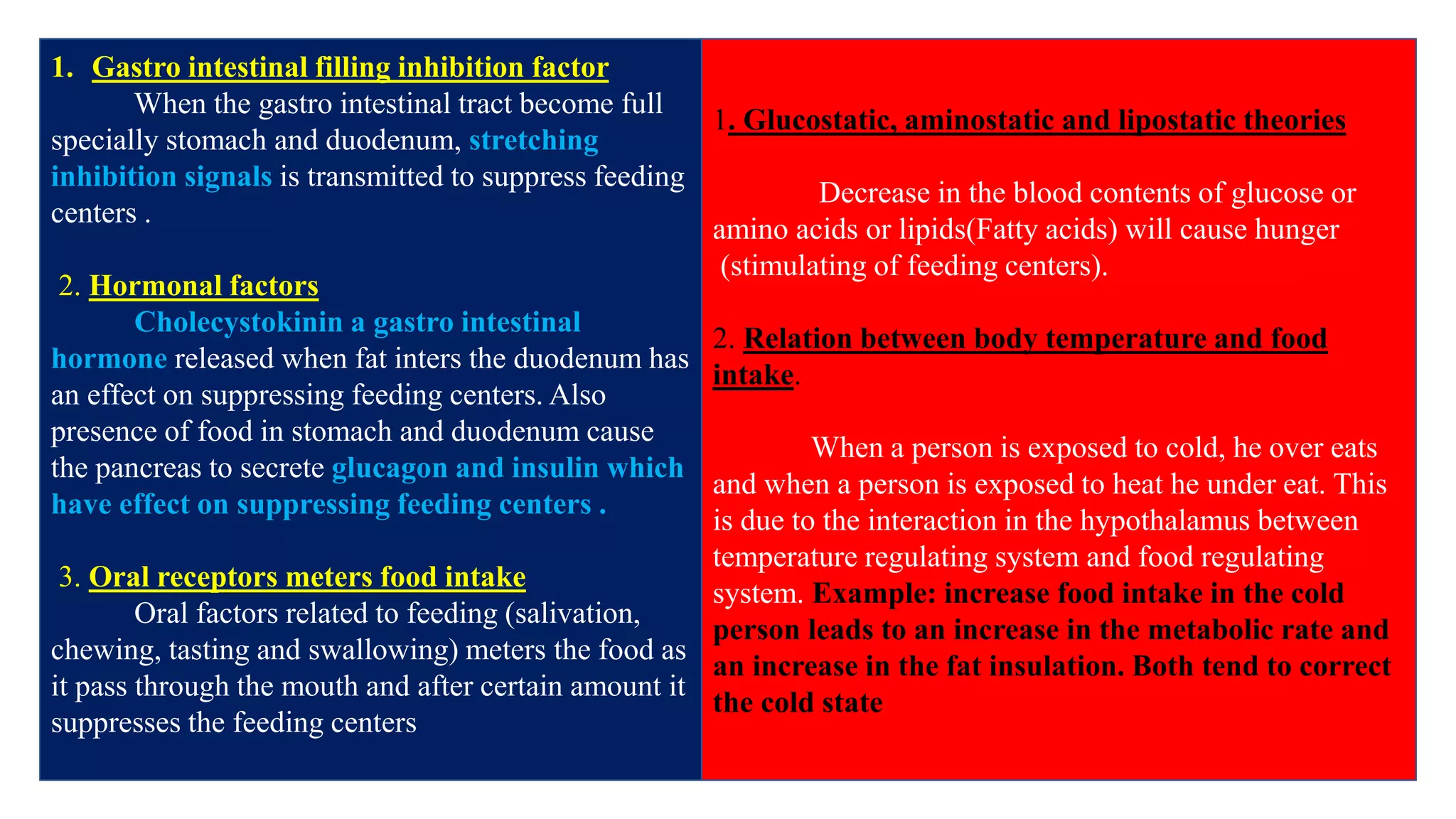
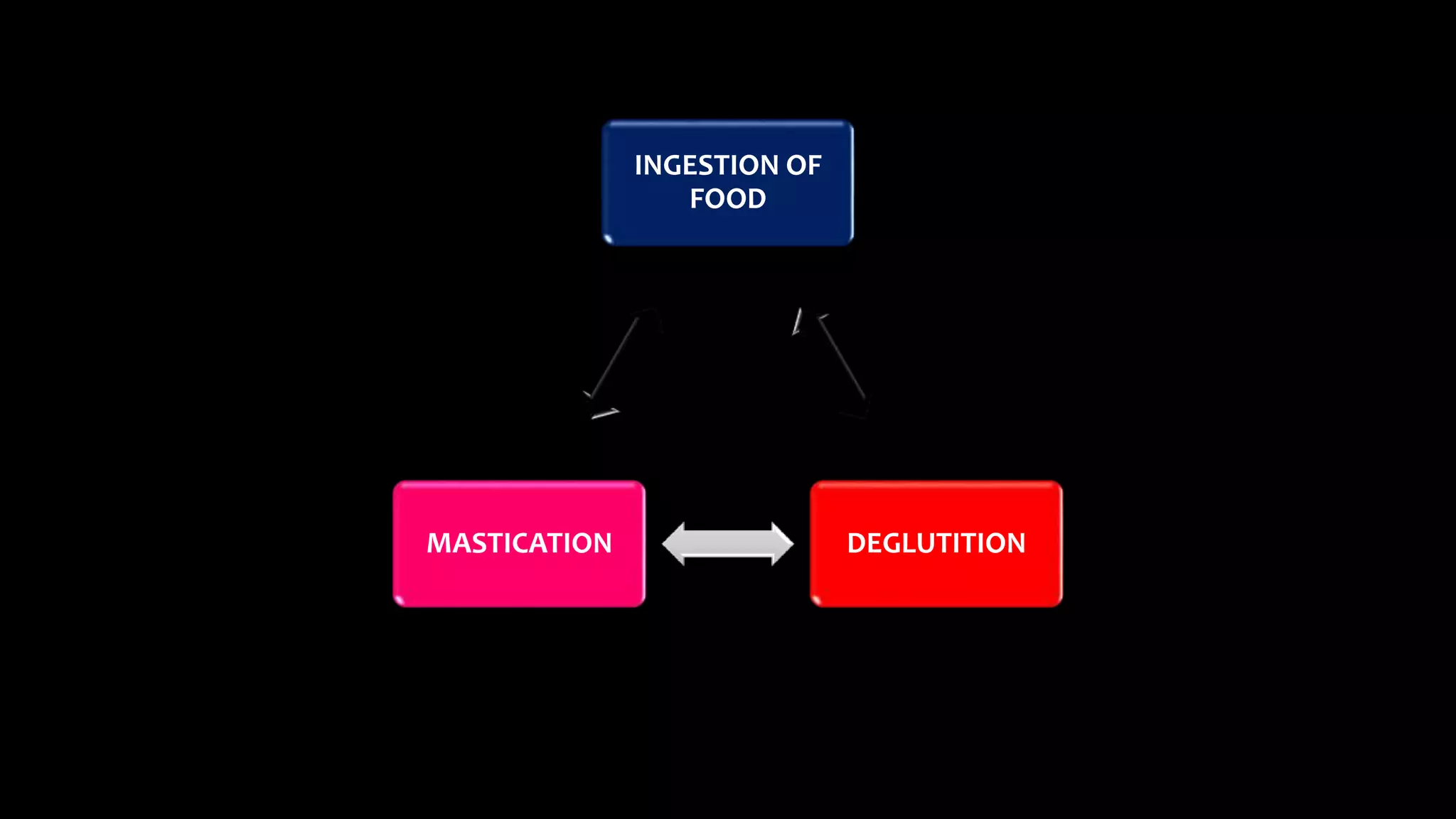
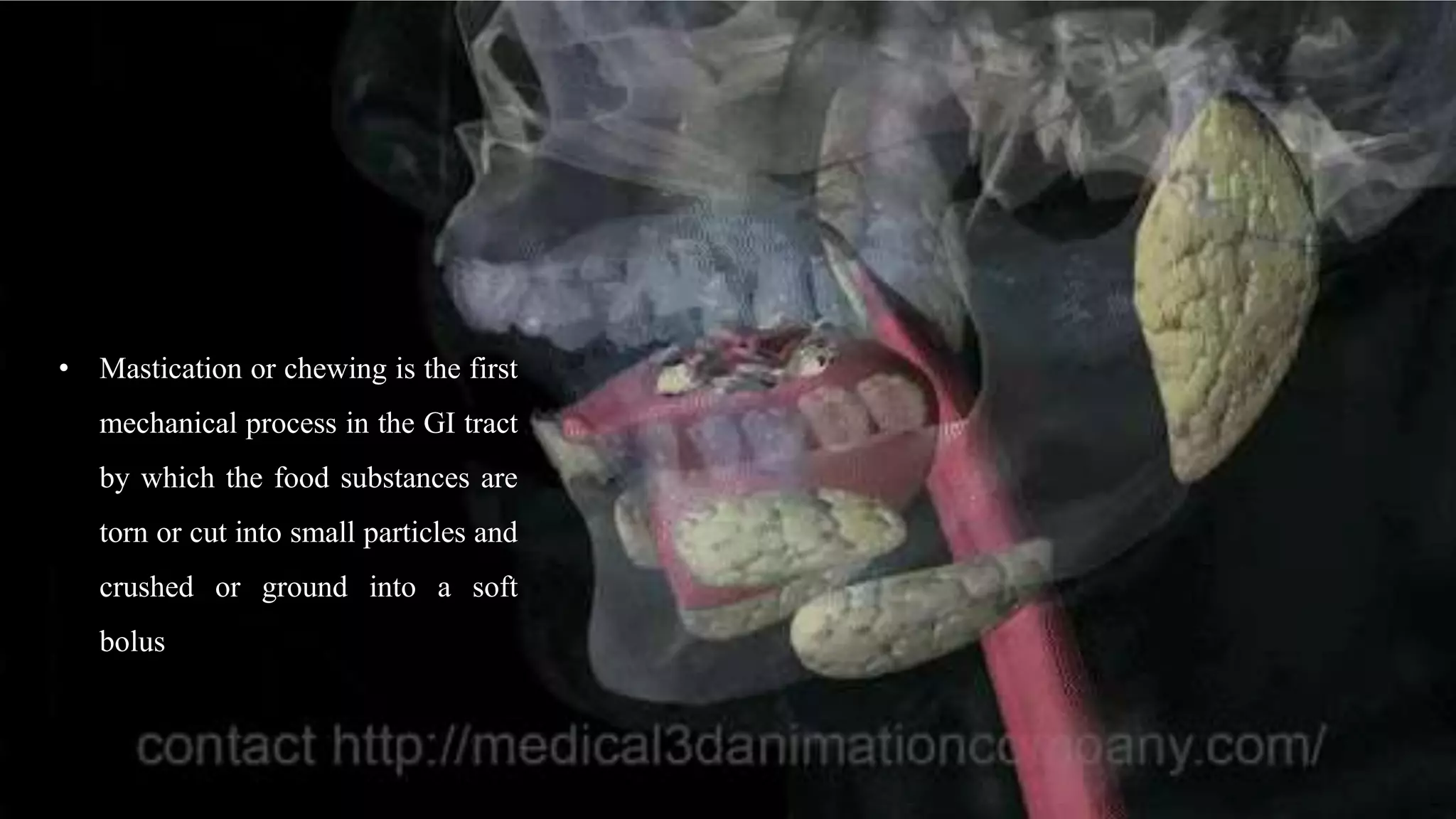
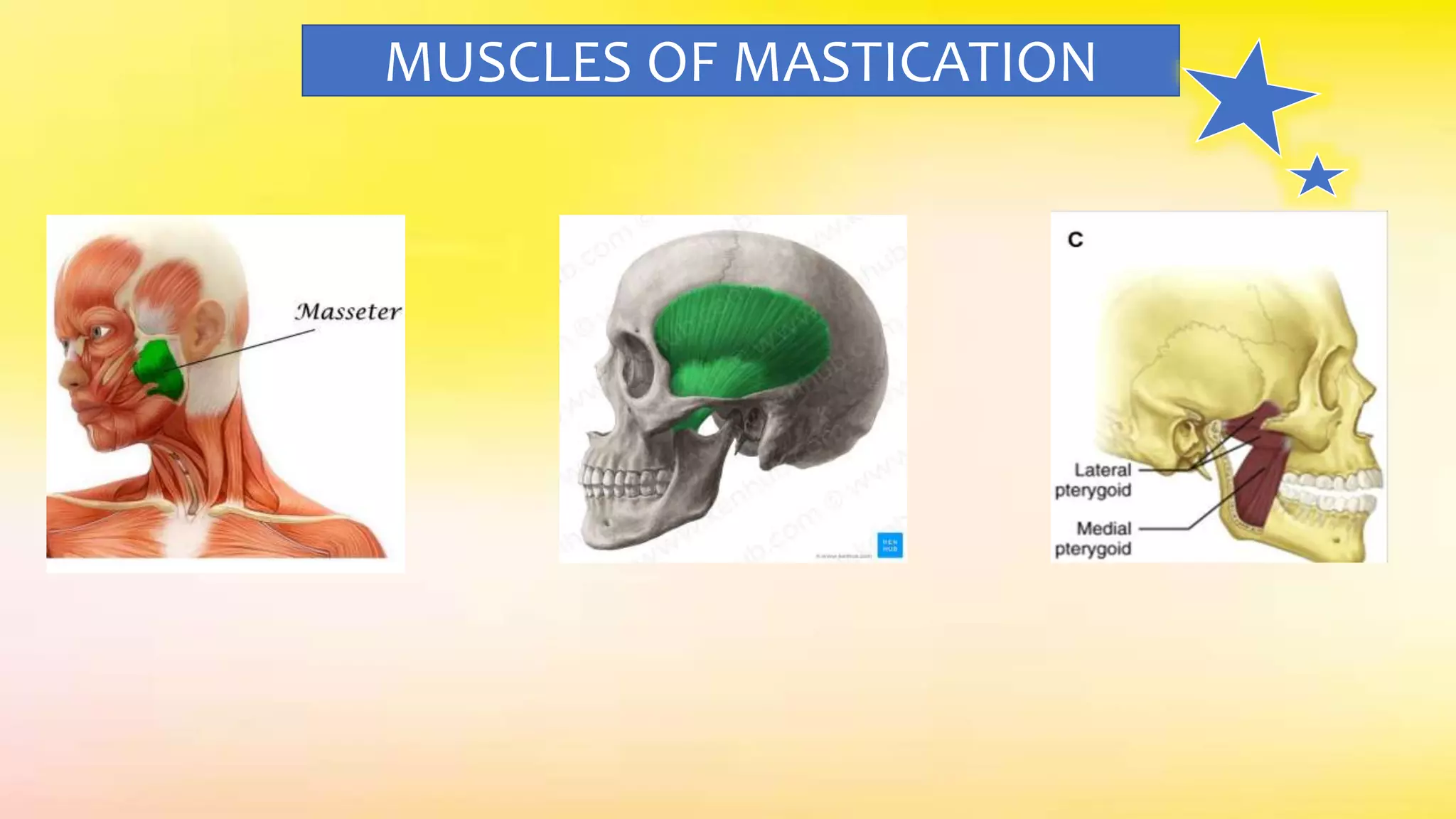
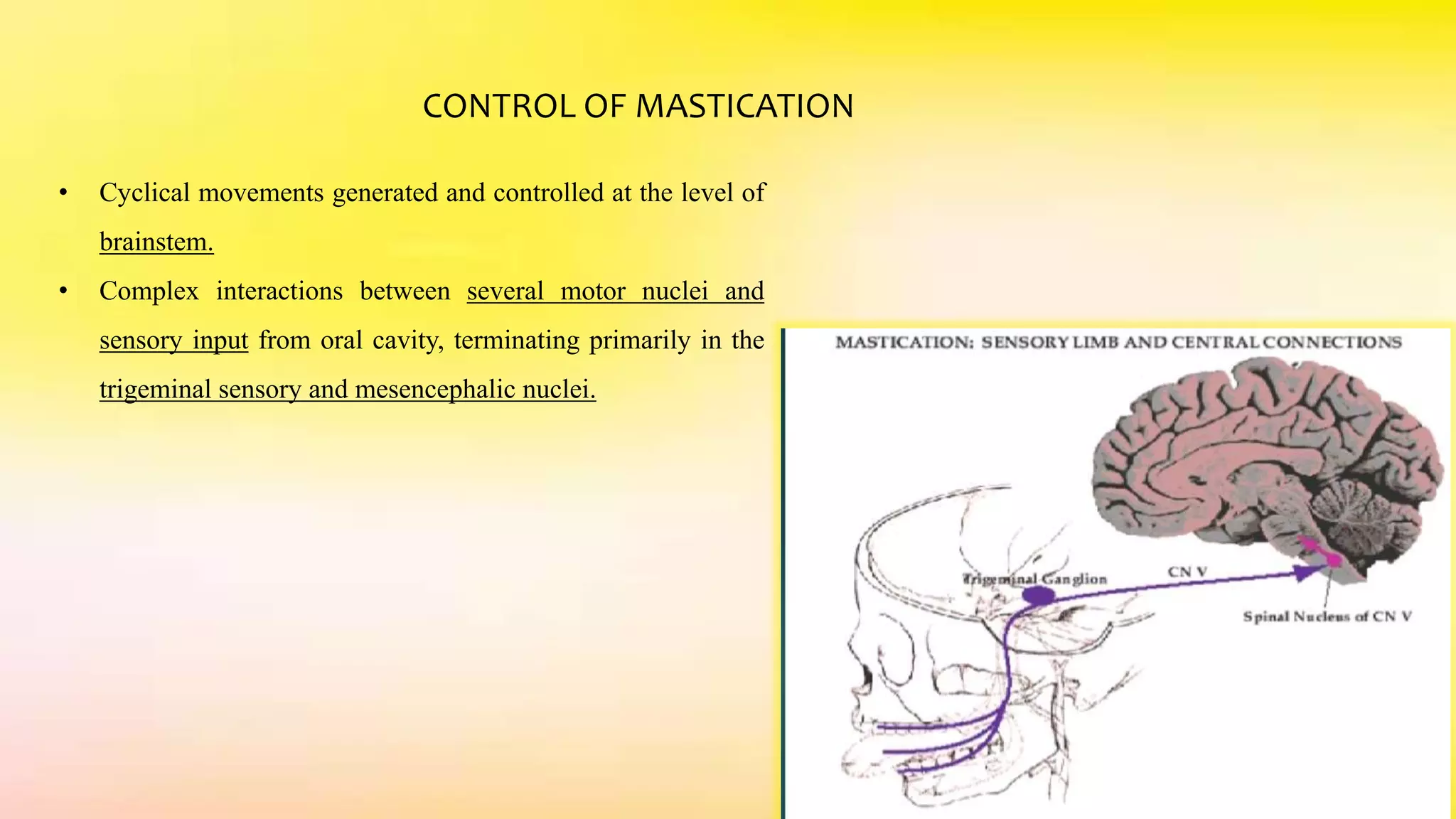
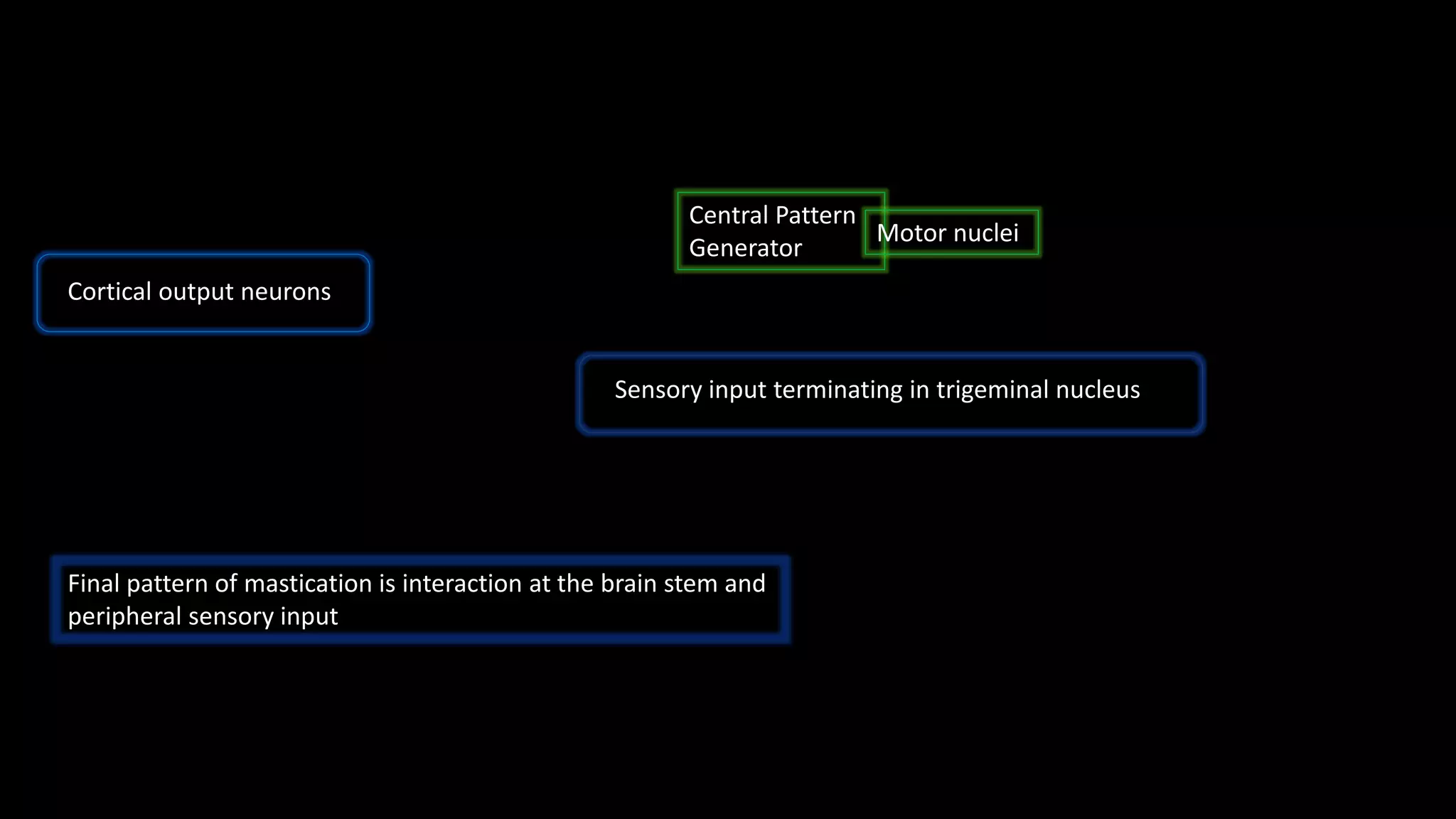
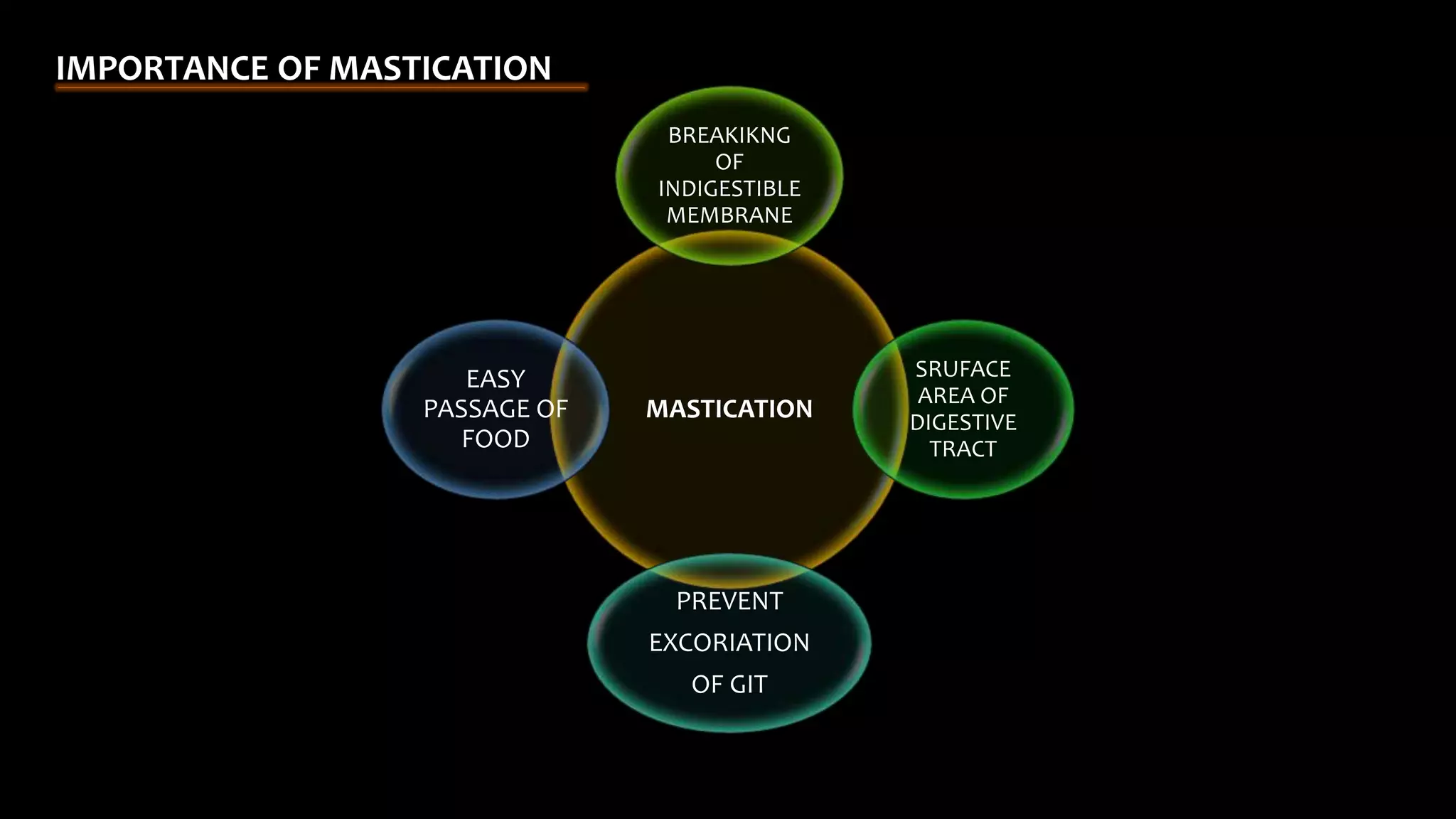
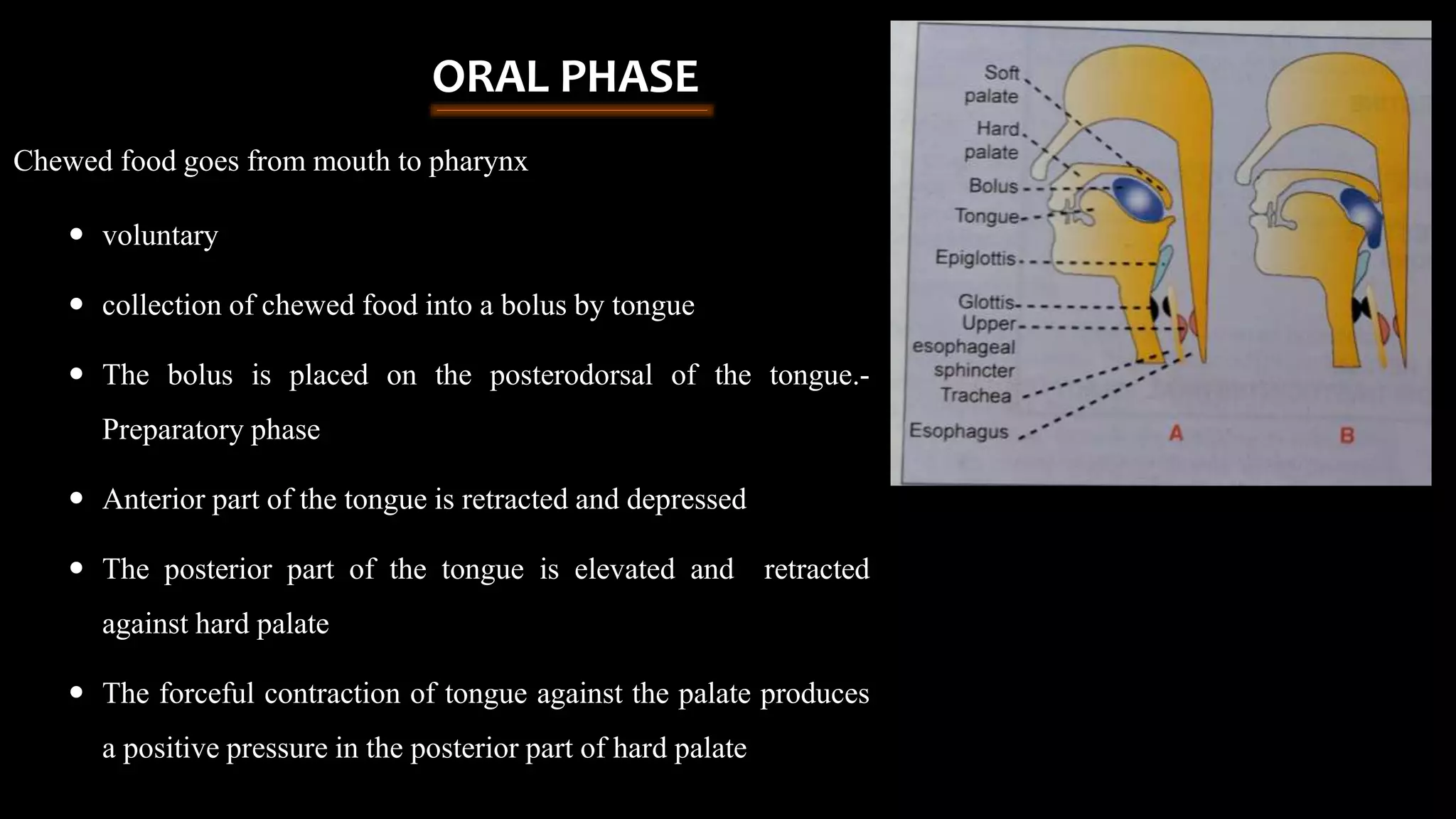
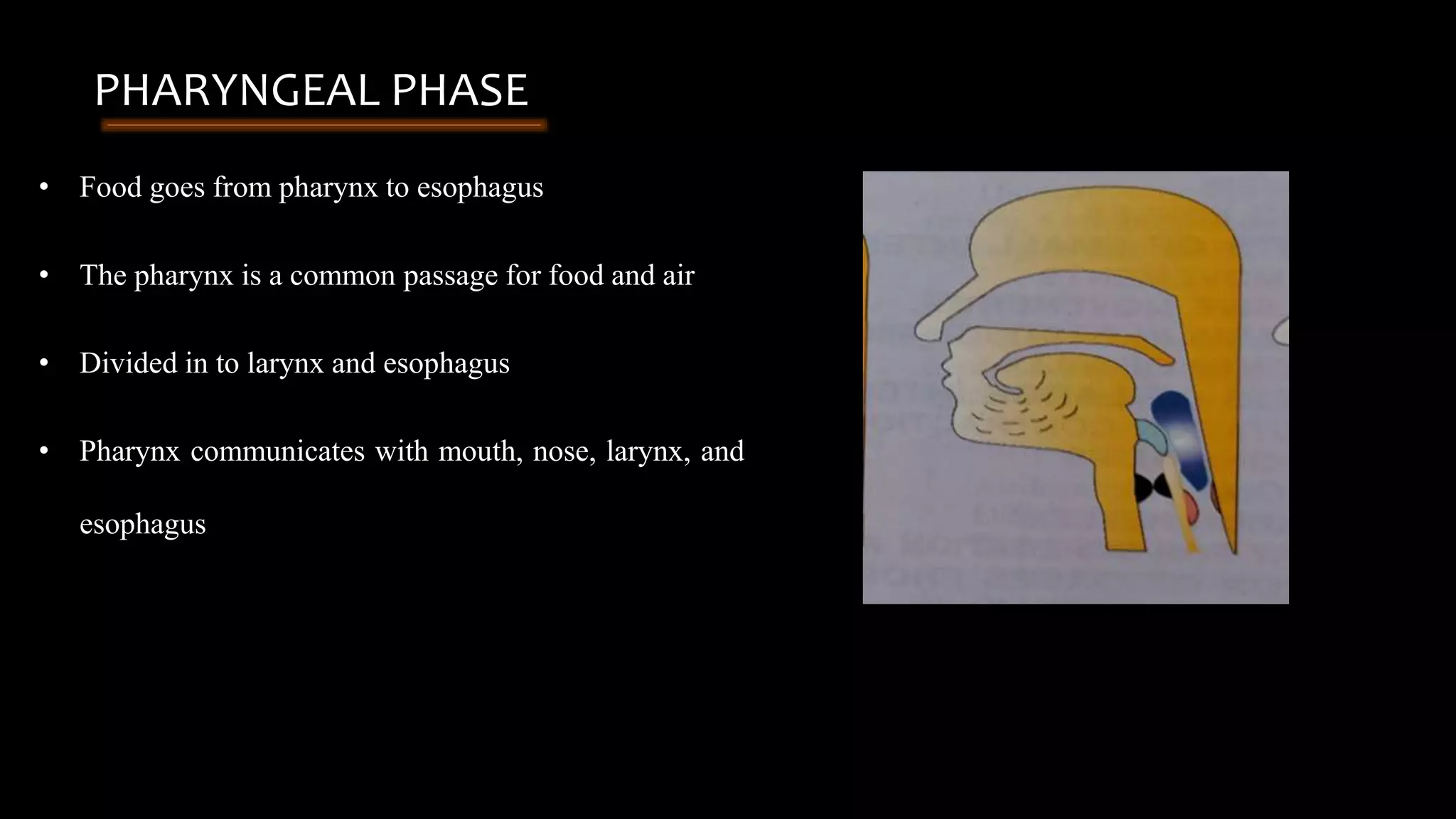
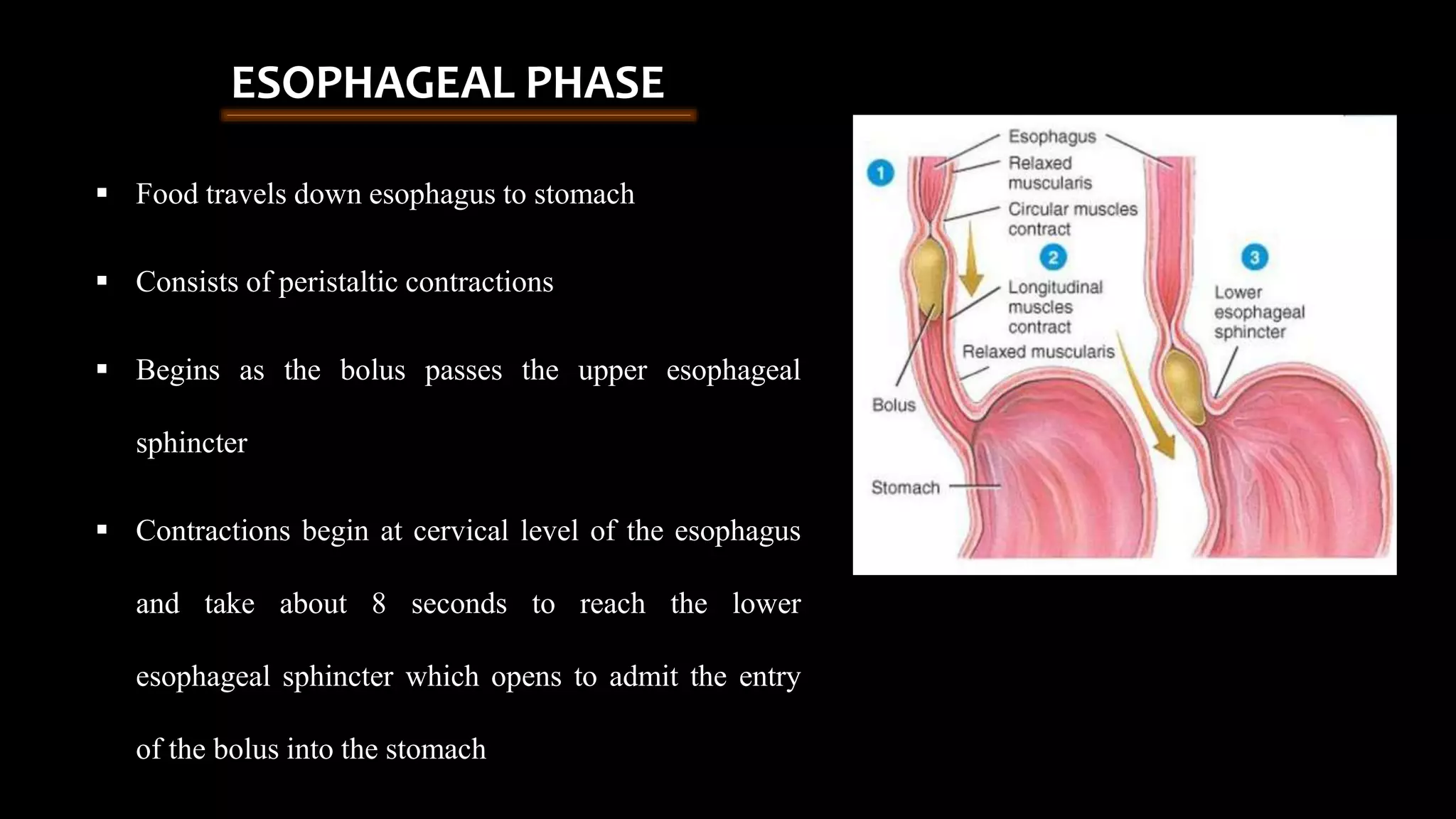
This document provides information about mastication and deglutition. It begins with an introduction to digestion and the digestive system. It then discusses factors that regulate food intake such as hunger and satiety centers in the hypothalamus. The document describes the process of mastication including the muscles involved, chewing strokes, and role of saliva. It also explains deglutition as the three phase process of food moving from the mouth to the esophagus. In summary, the document outlines the physiological processes of chewing, swallowing, and their roles in breaking down food for digestion.