1) Mastication involves the chewing and grinding of food using the teeth and muscles of mastication. As food is broken down, it is mixed with saliva and prepared for swallowing.
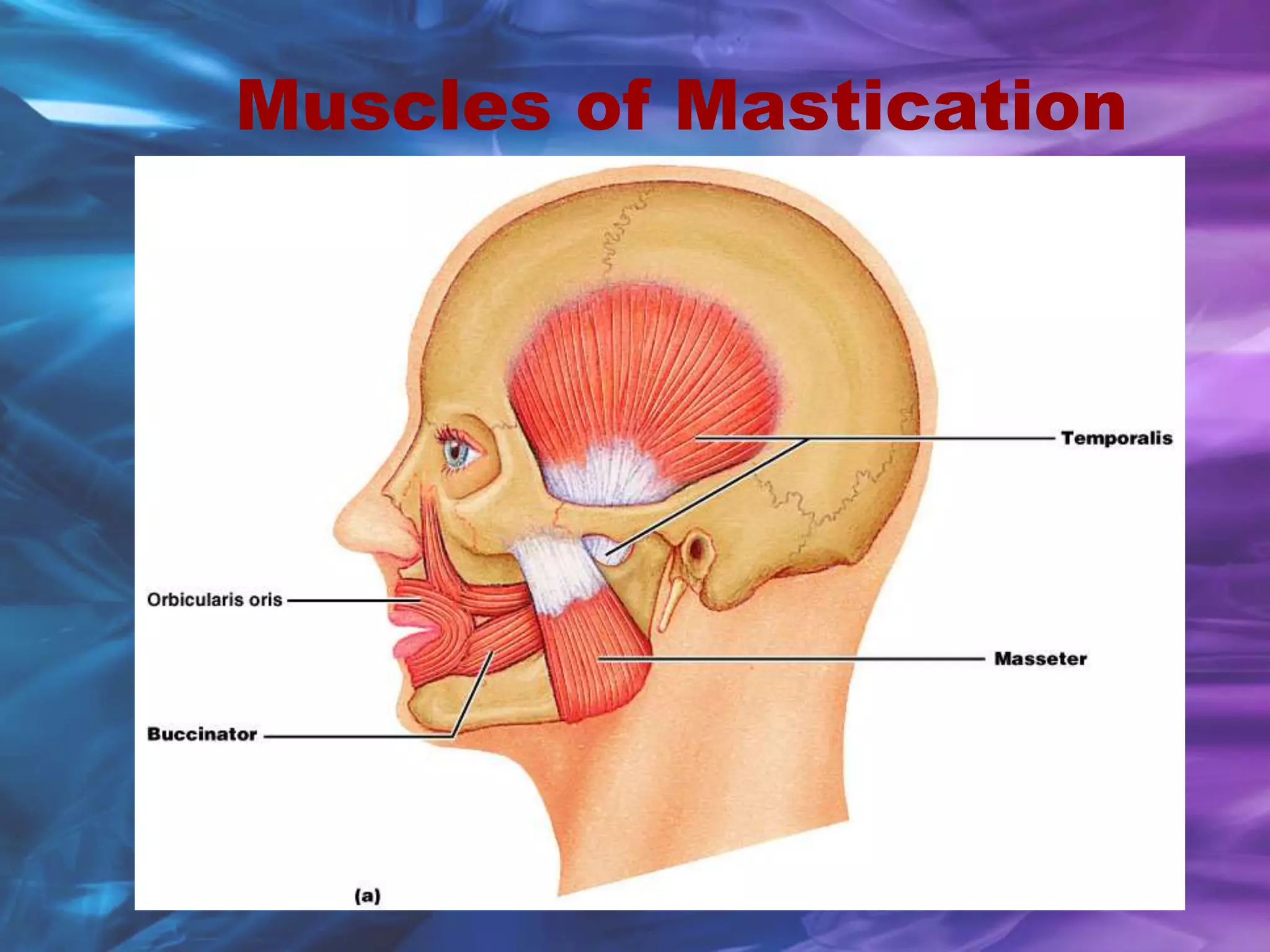
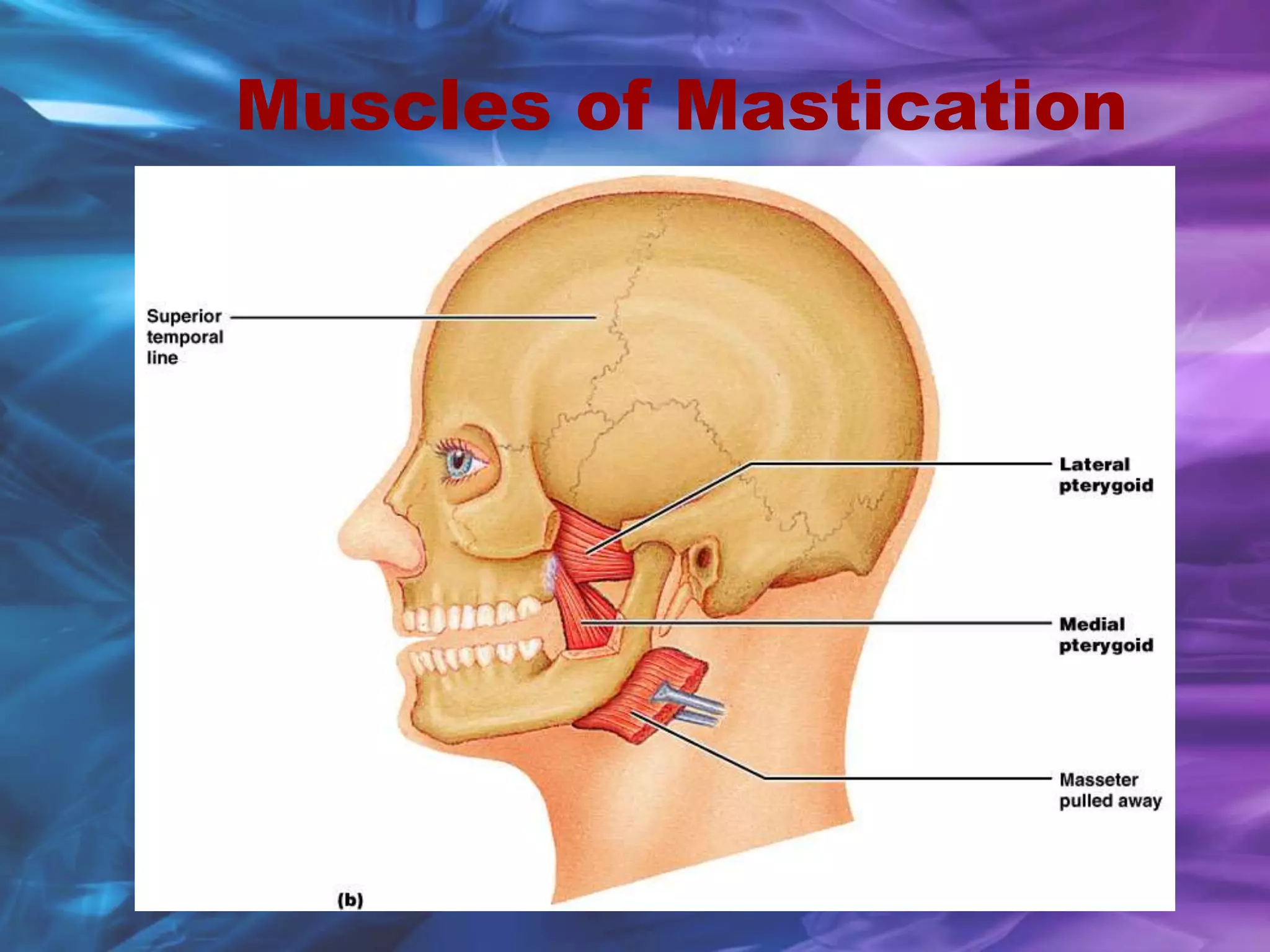
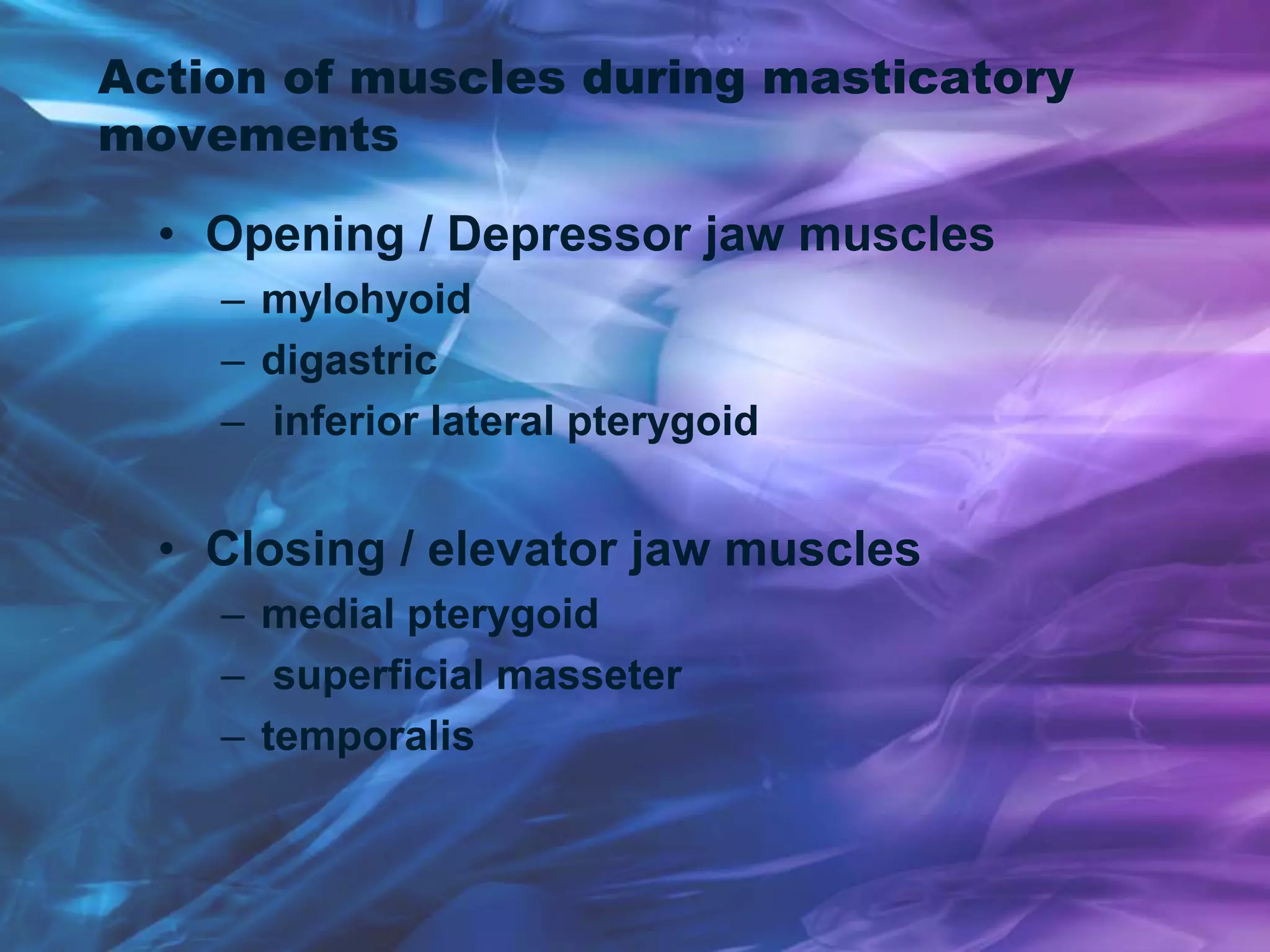
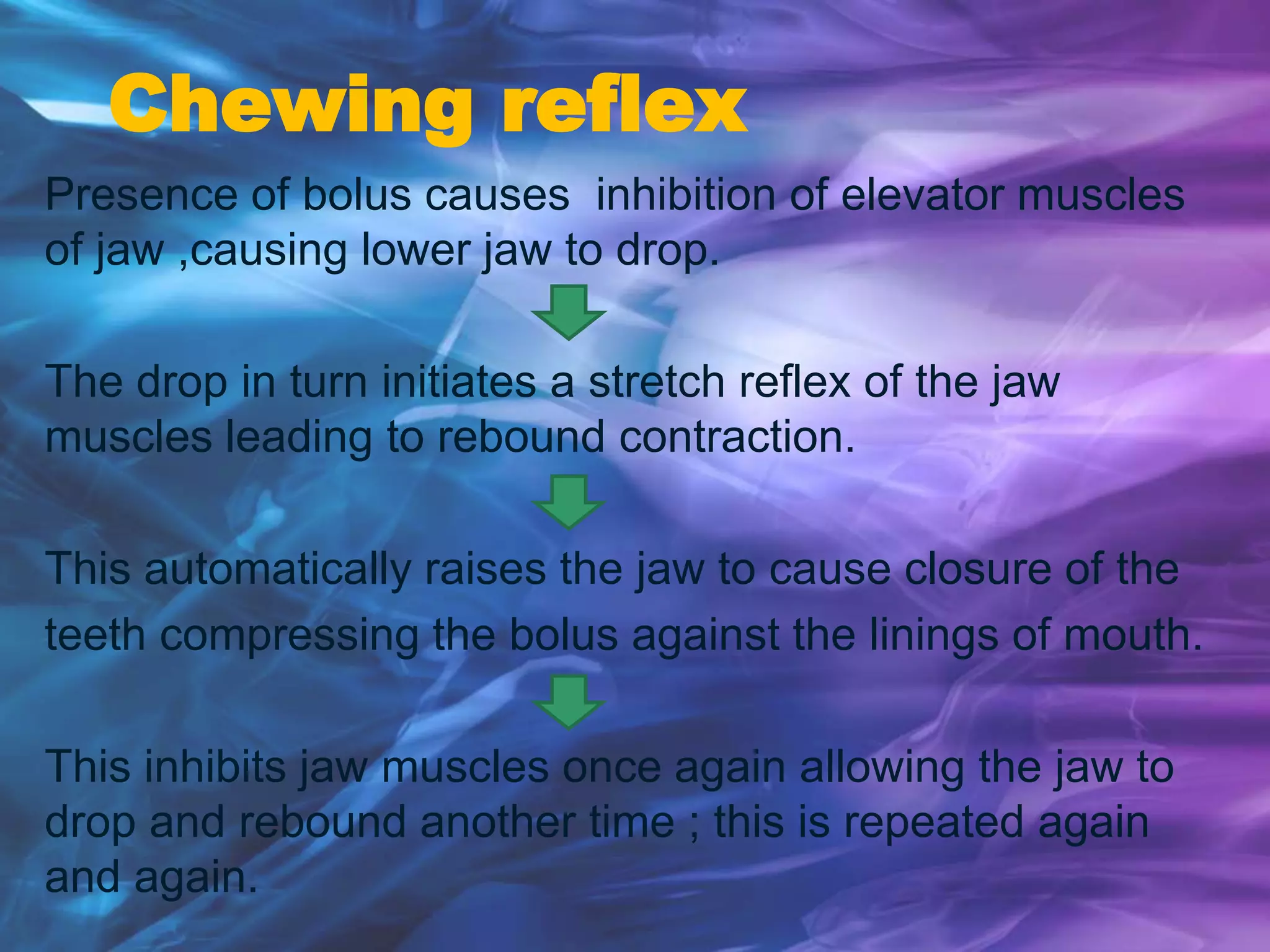
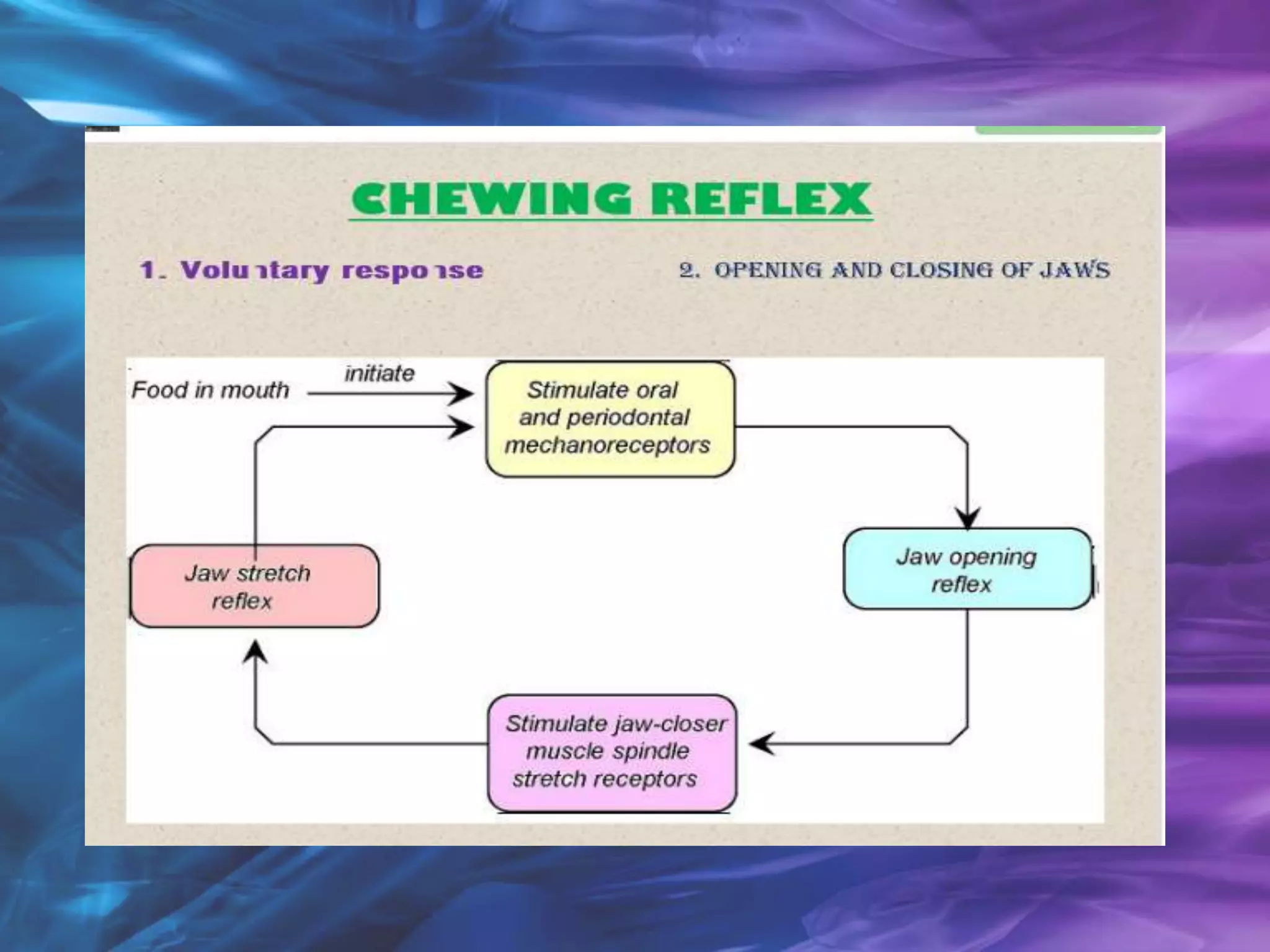
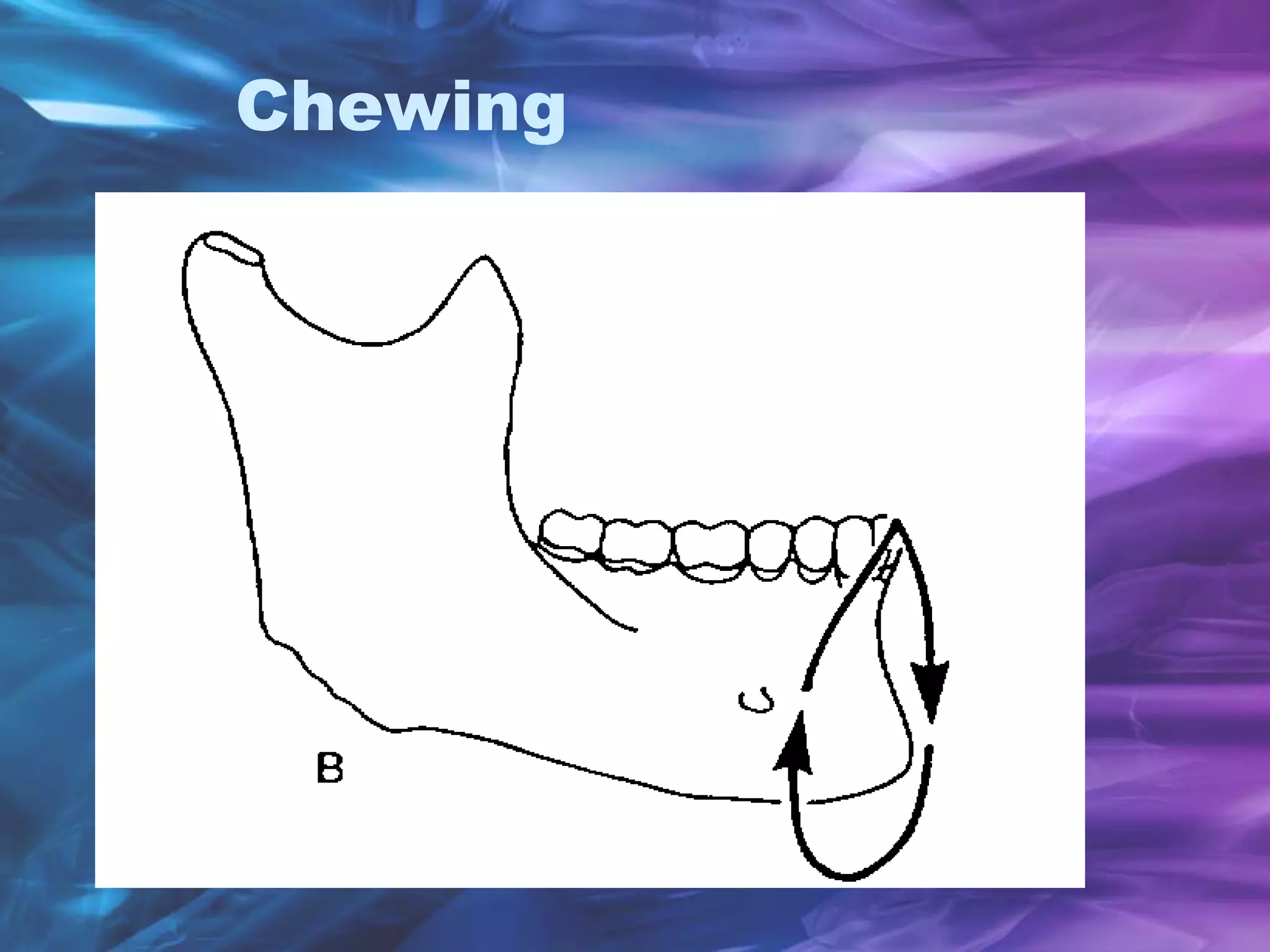
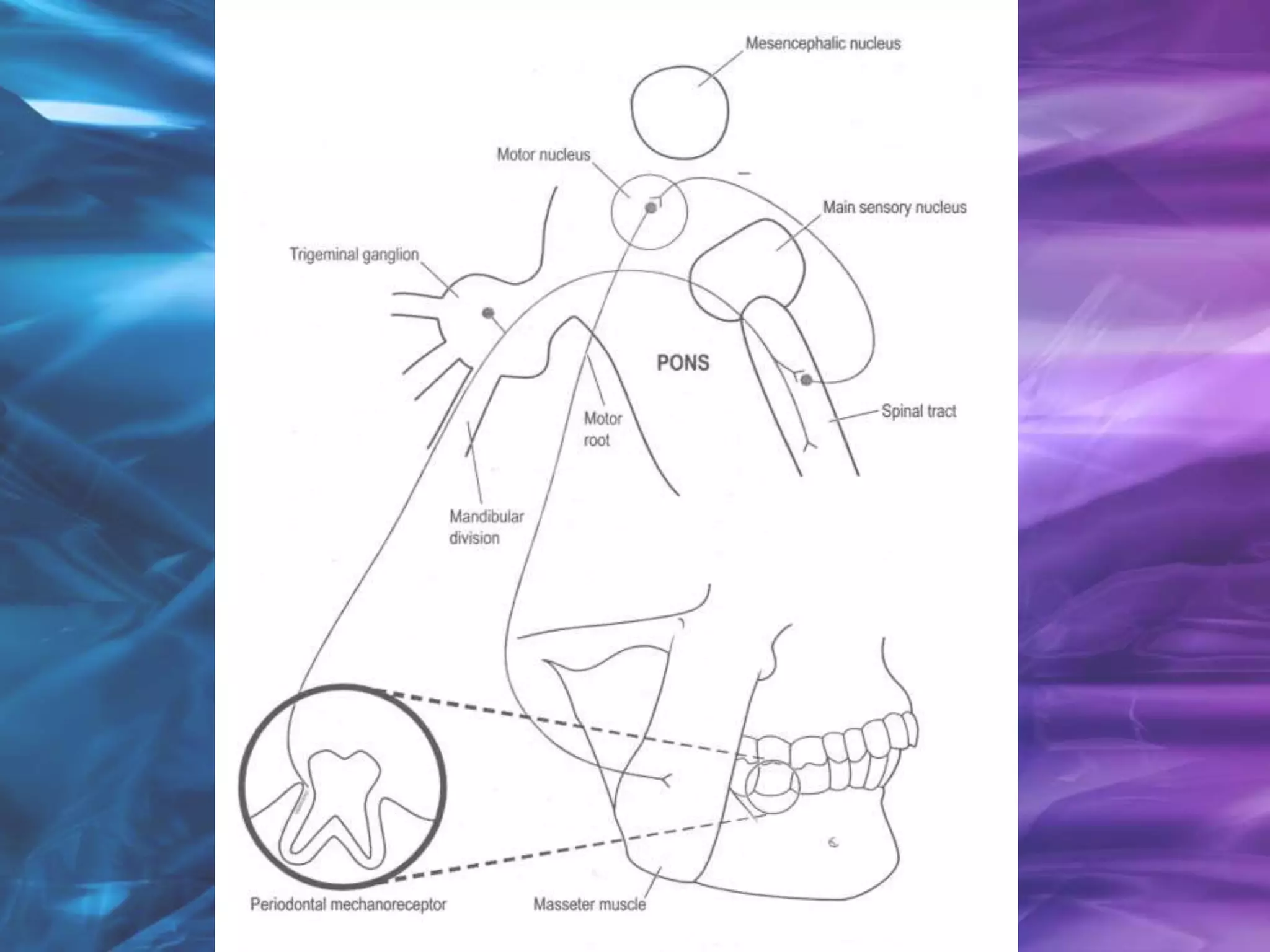
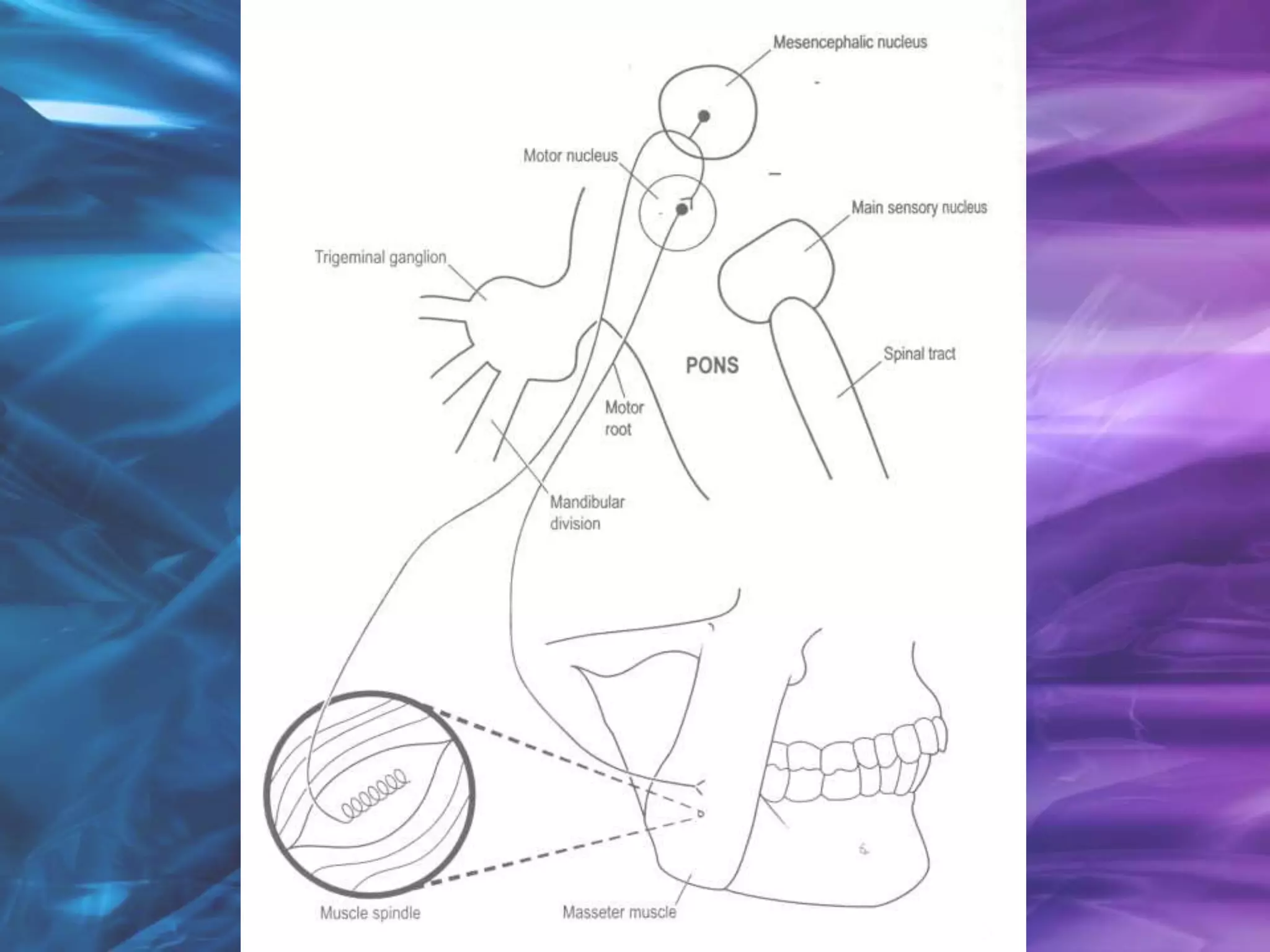
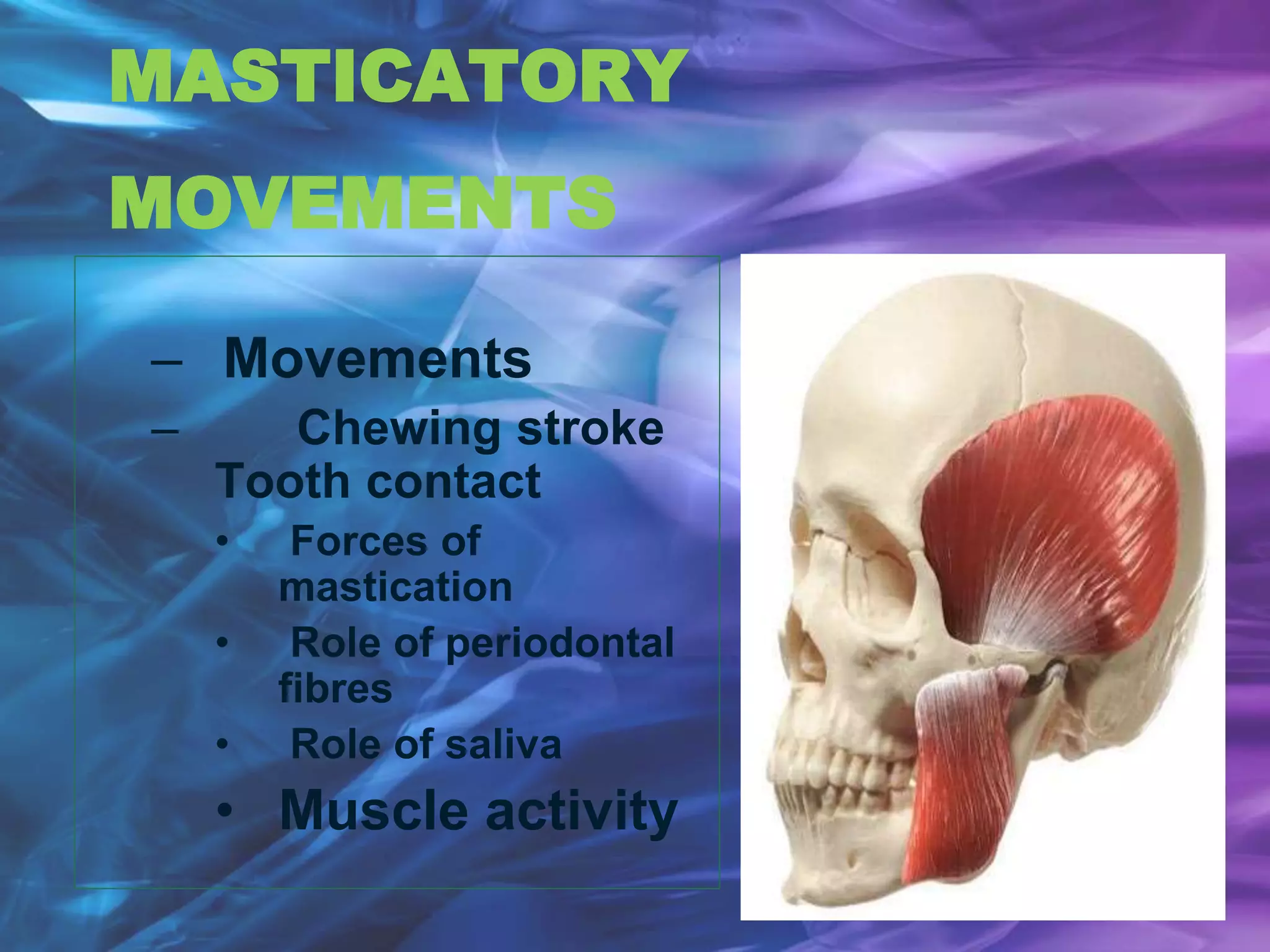
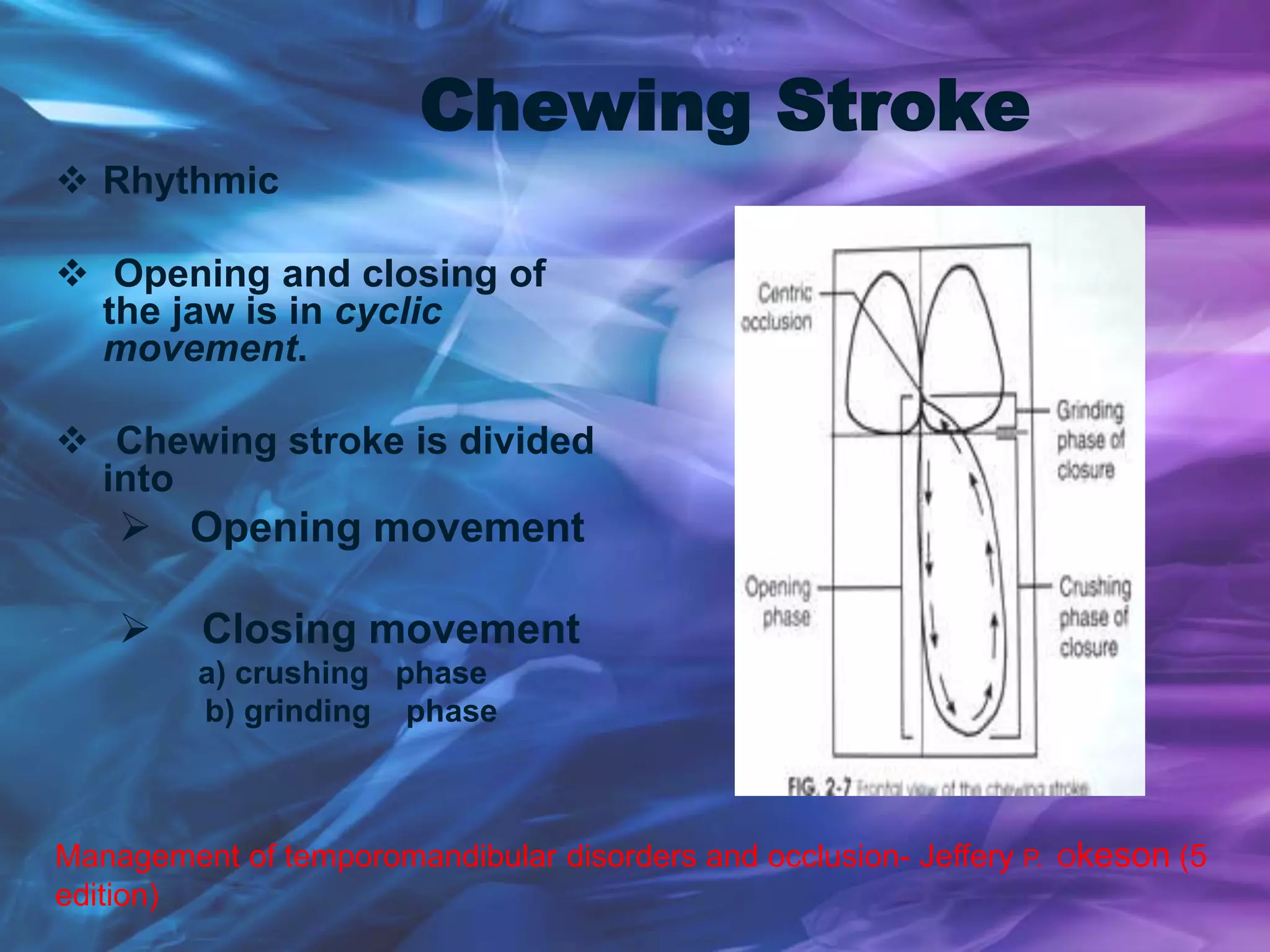
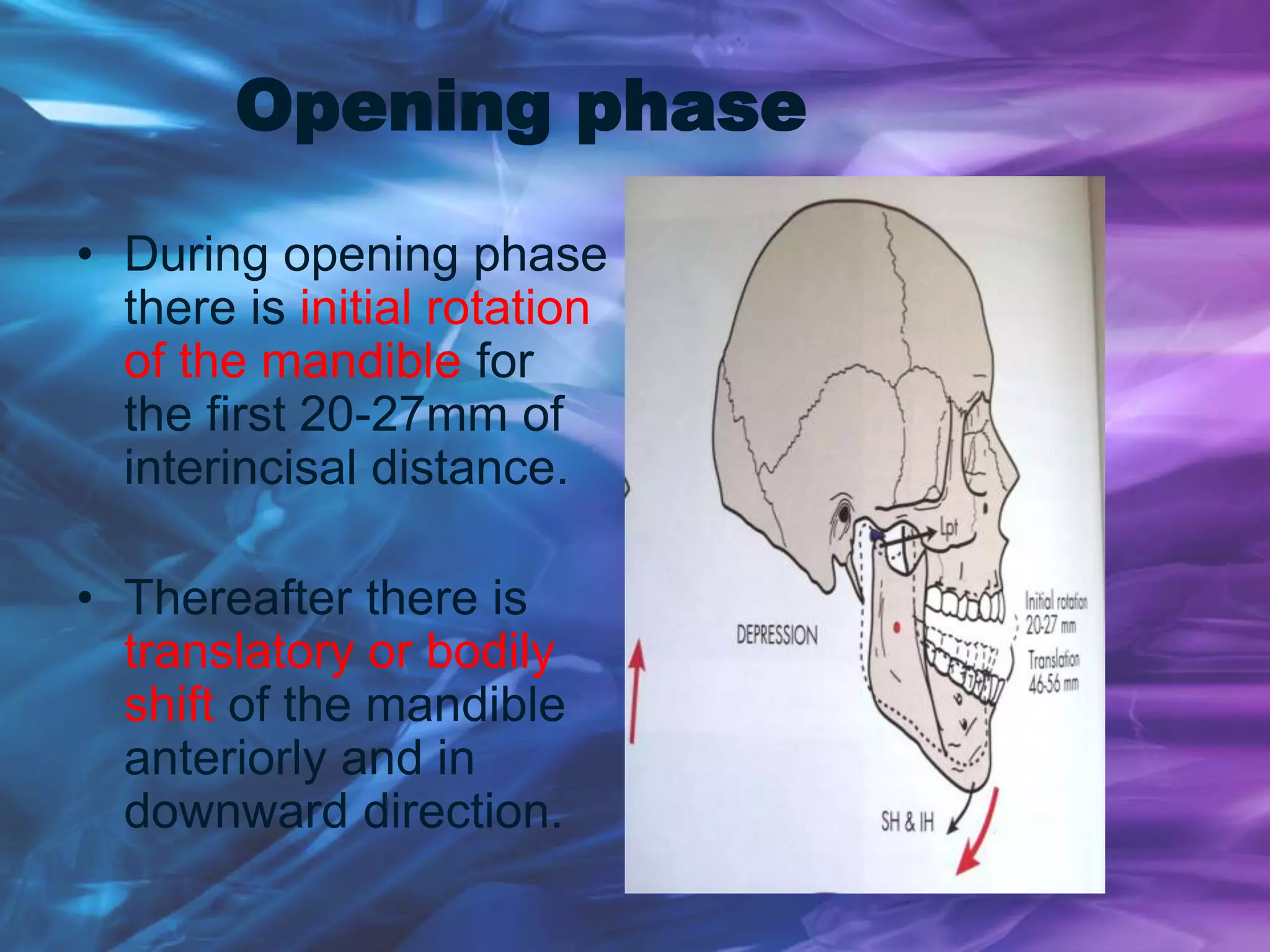
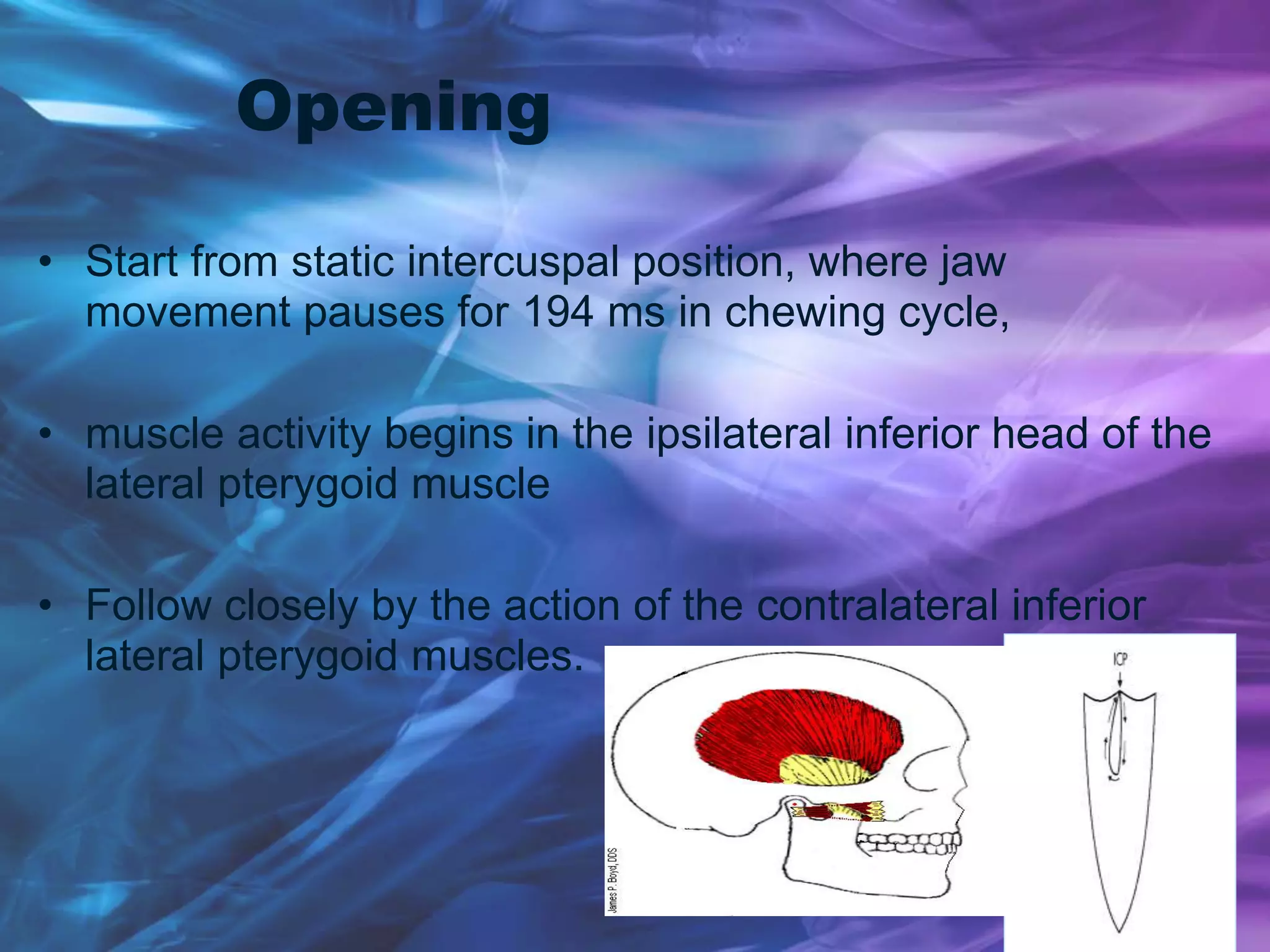
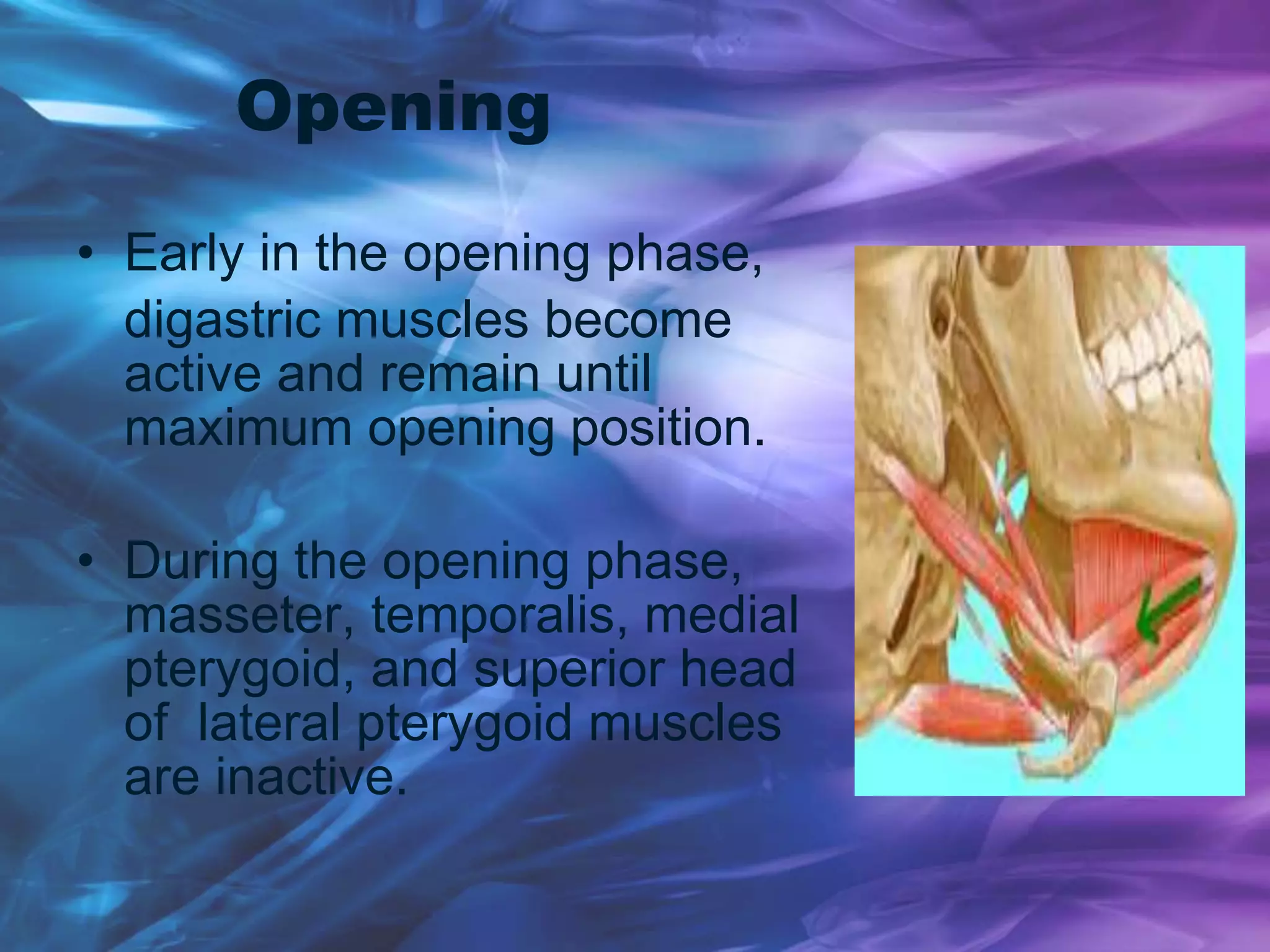
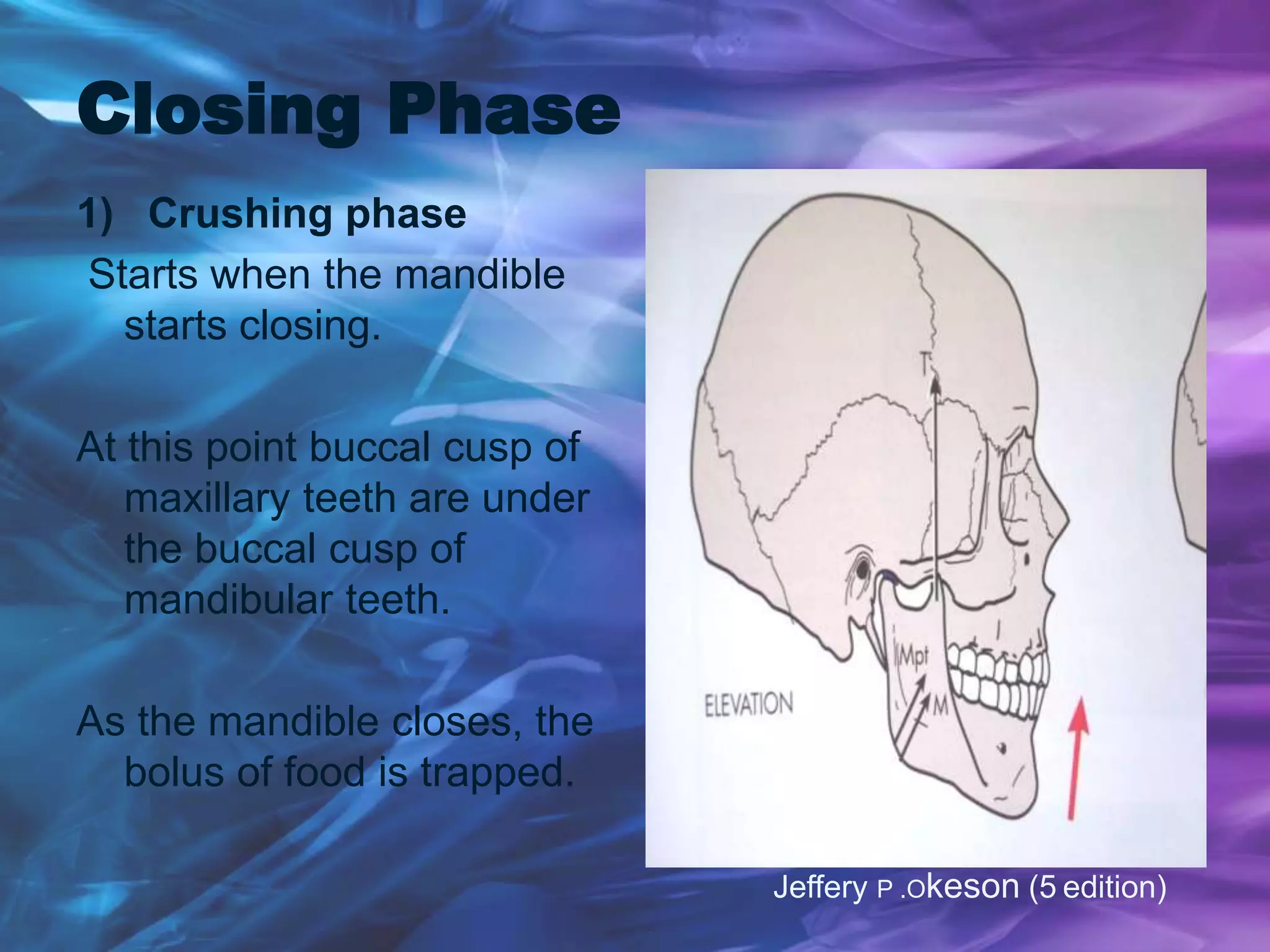
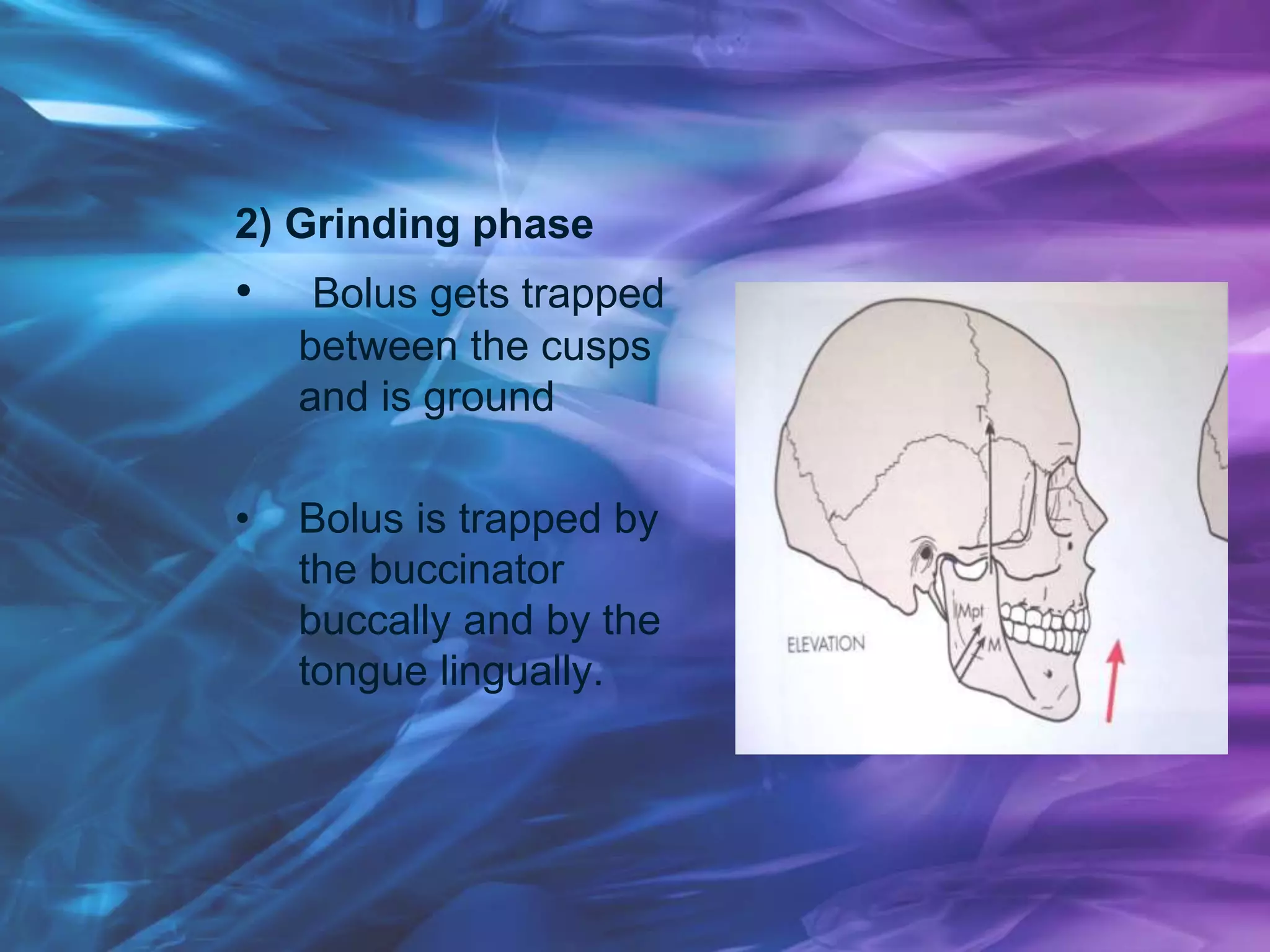
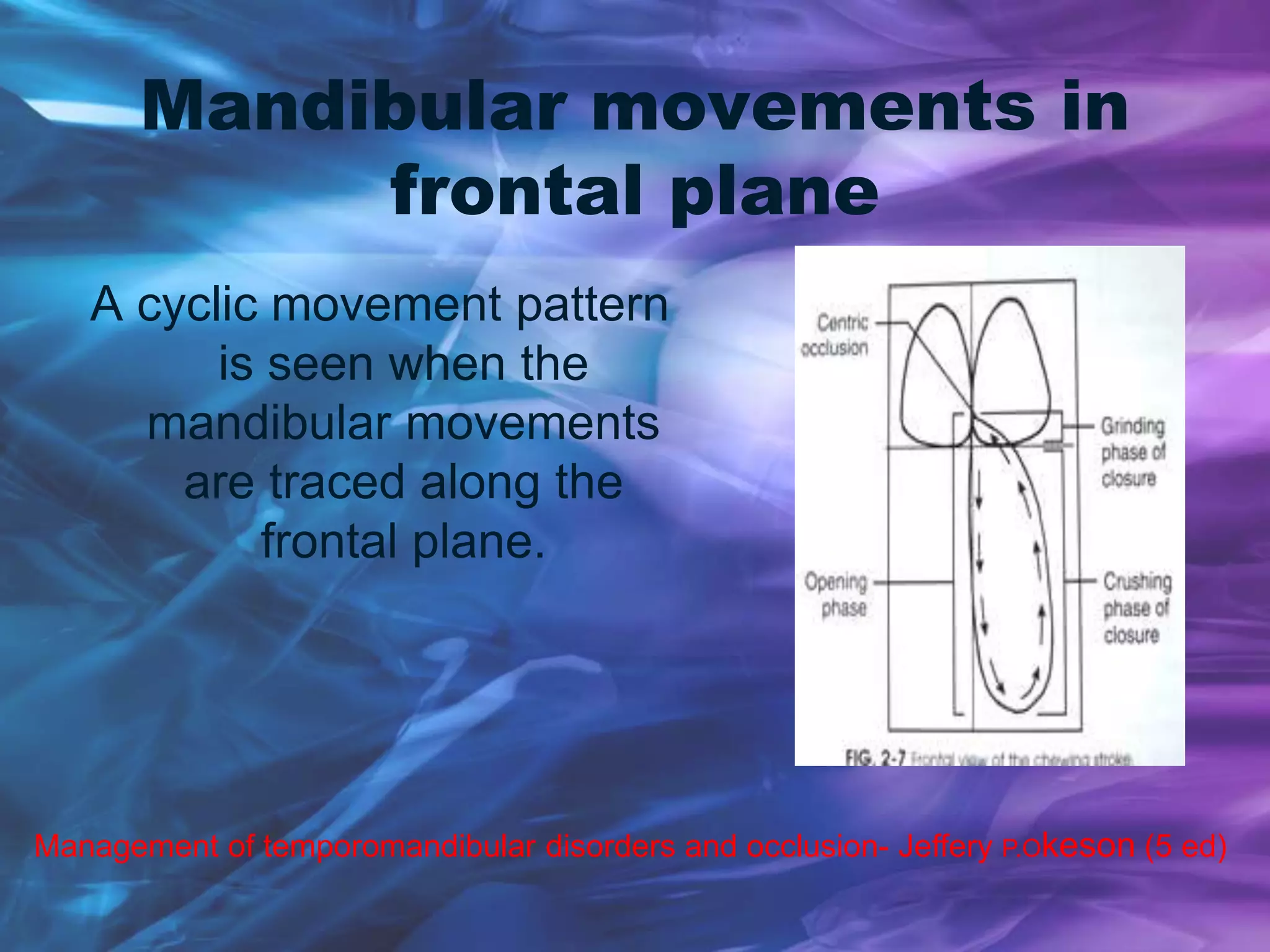
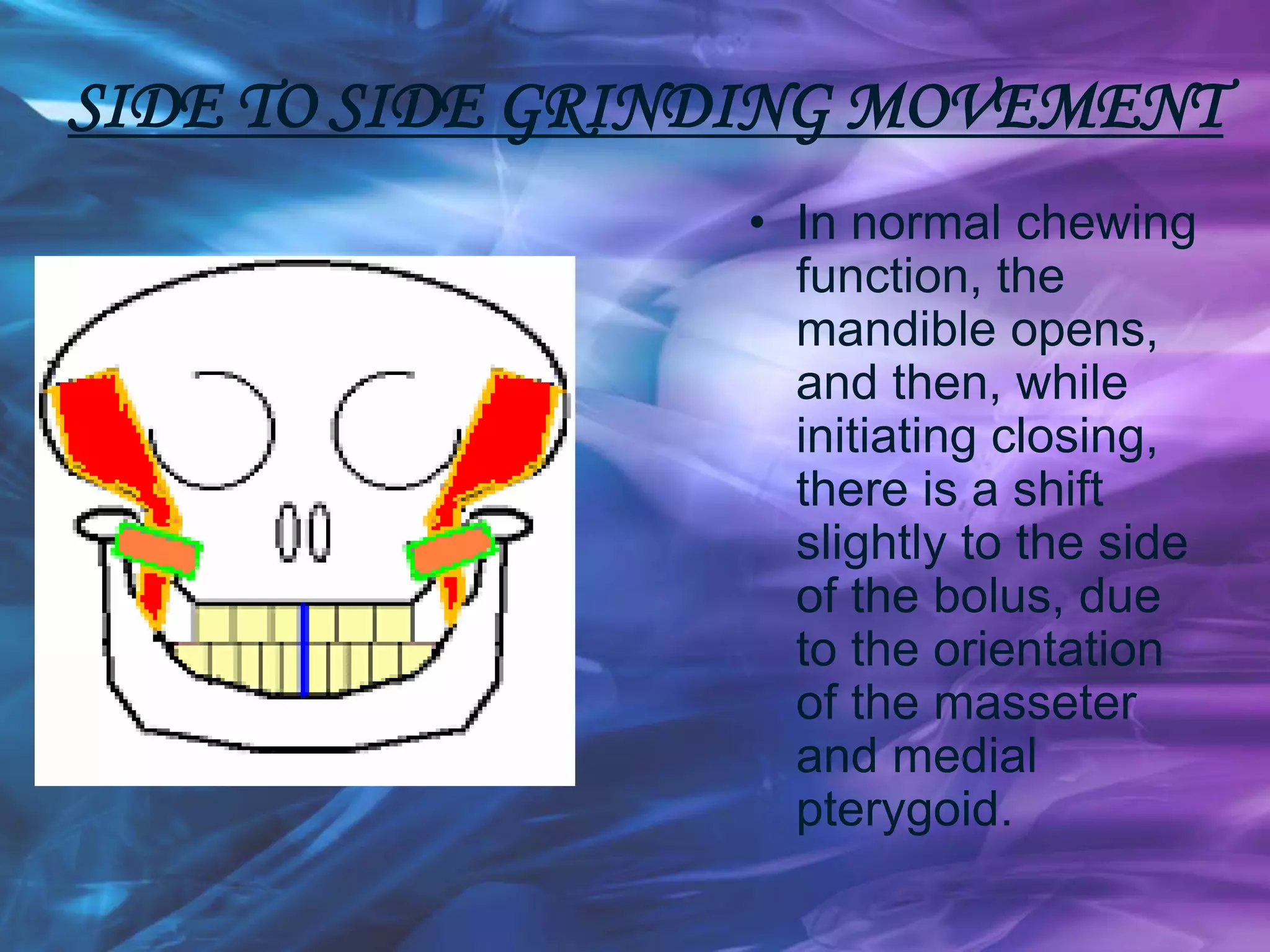
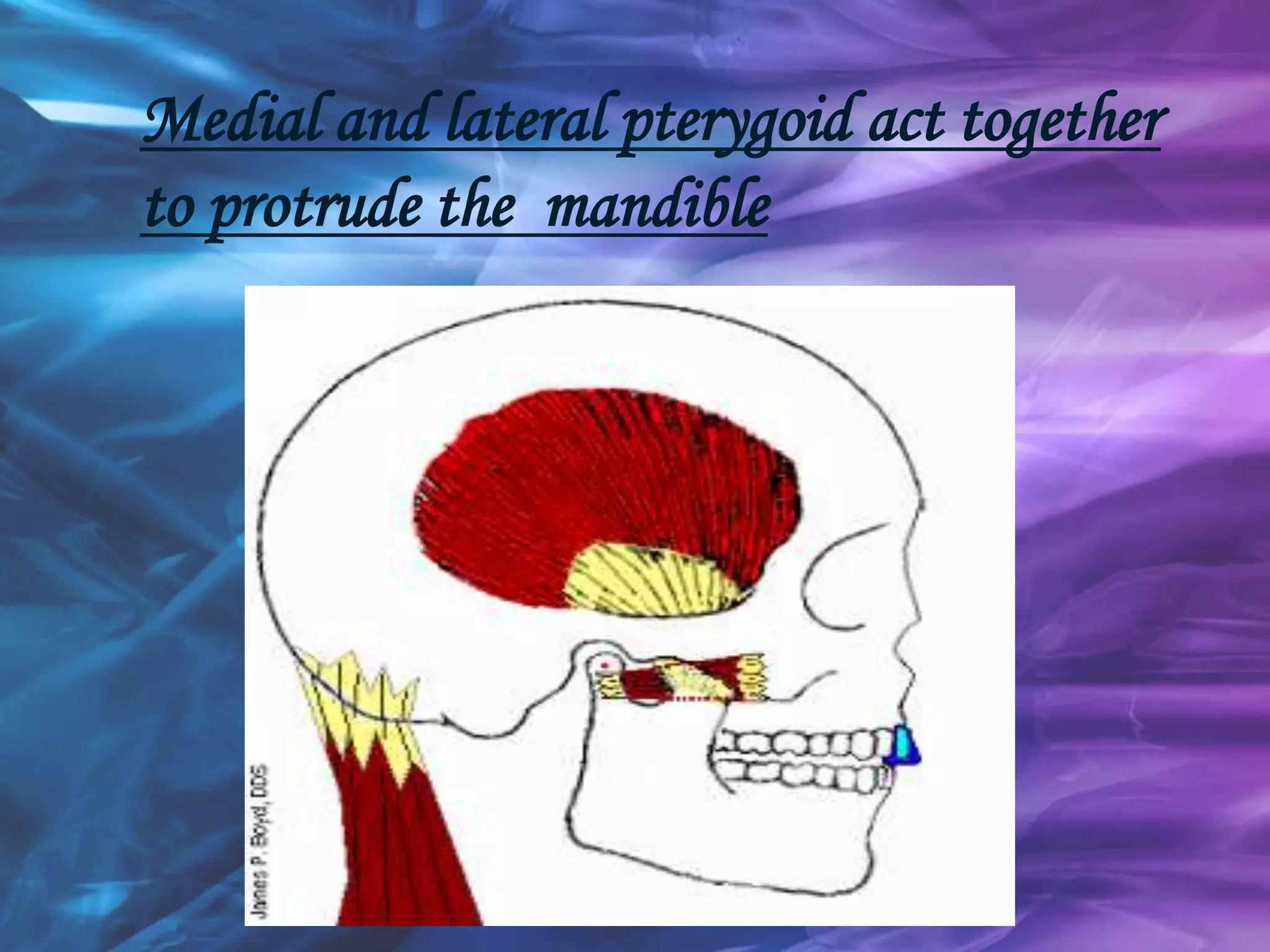
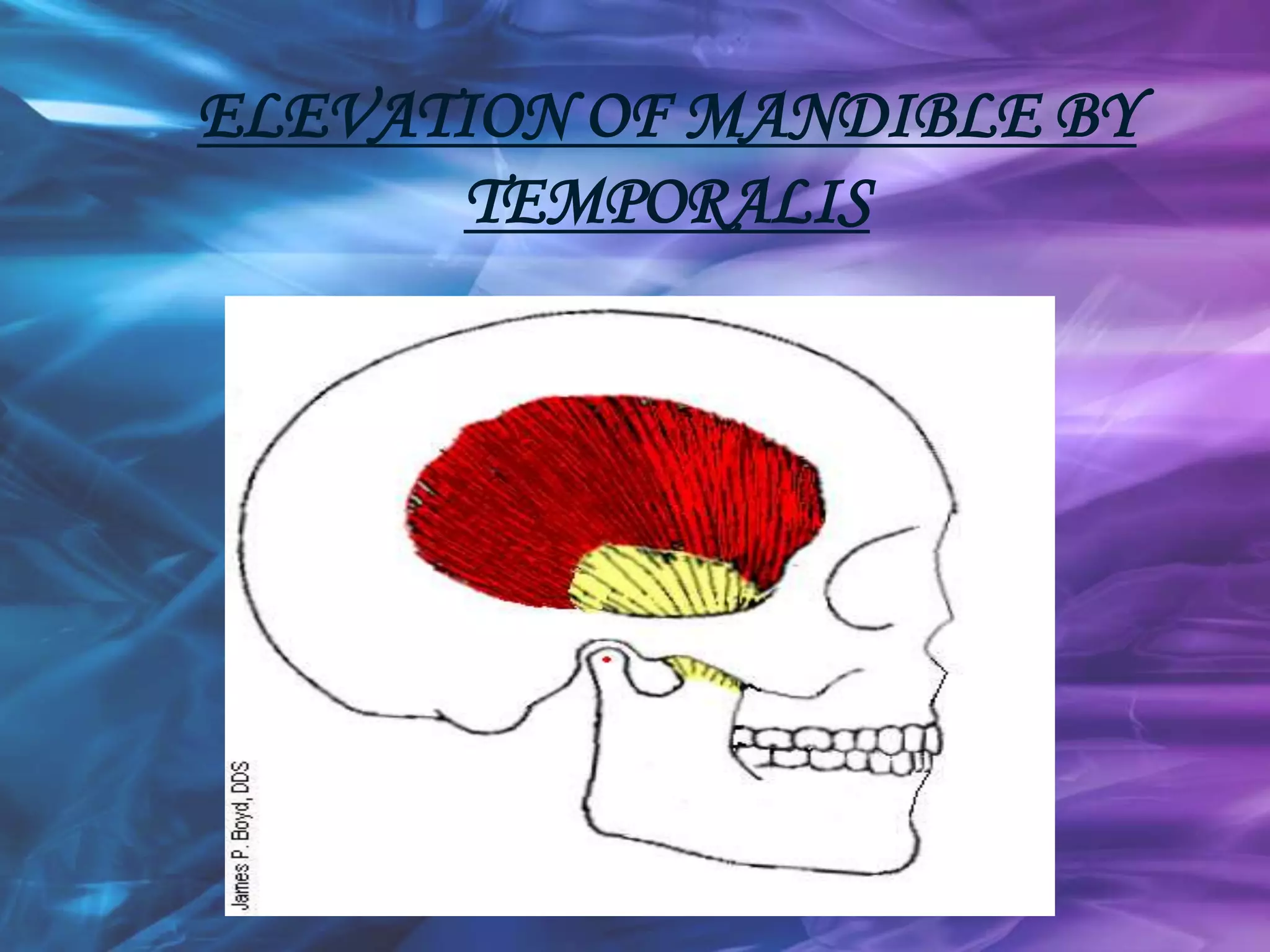
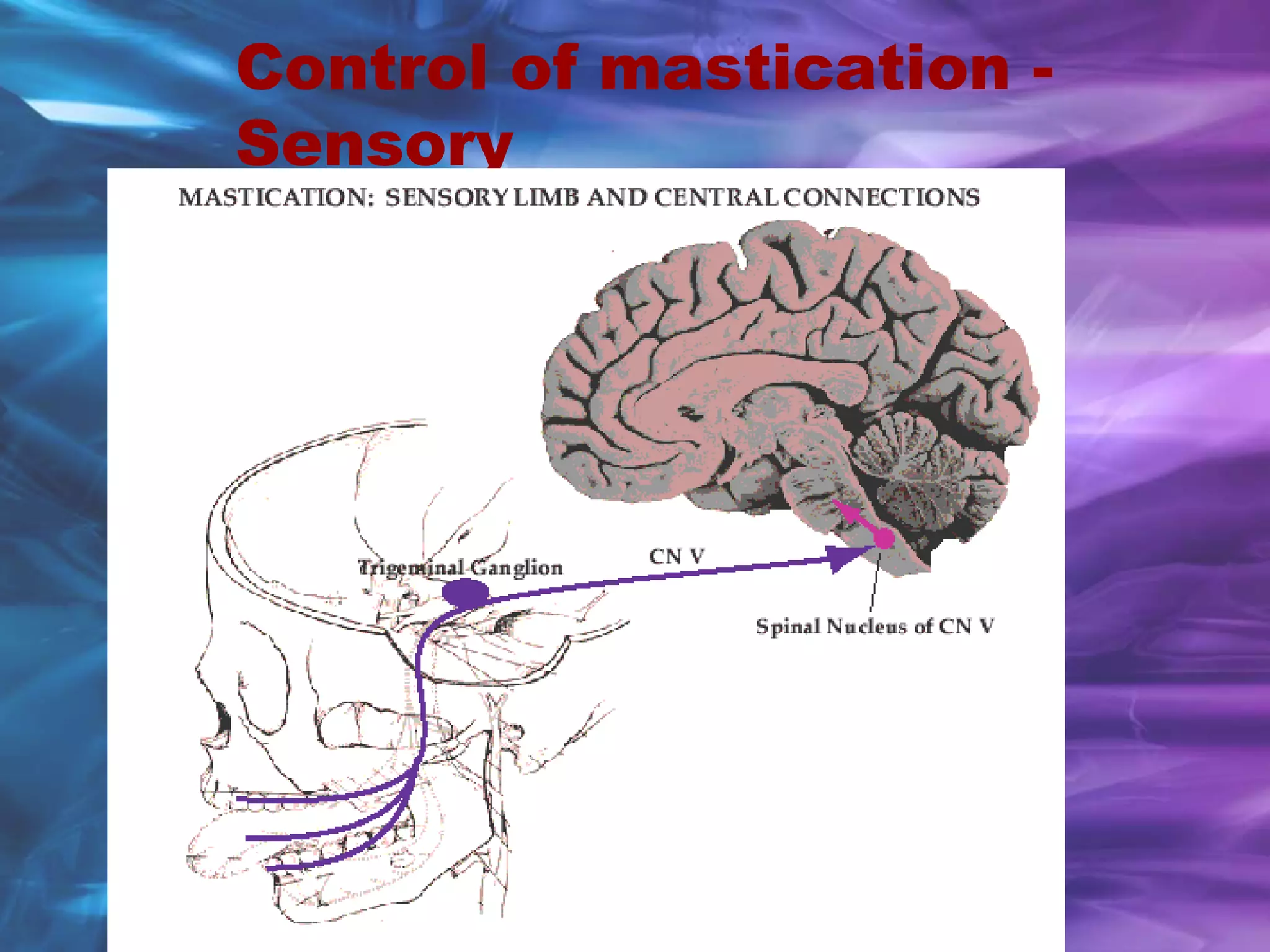
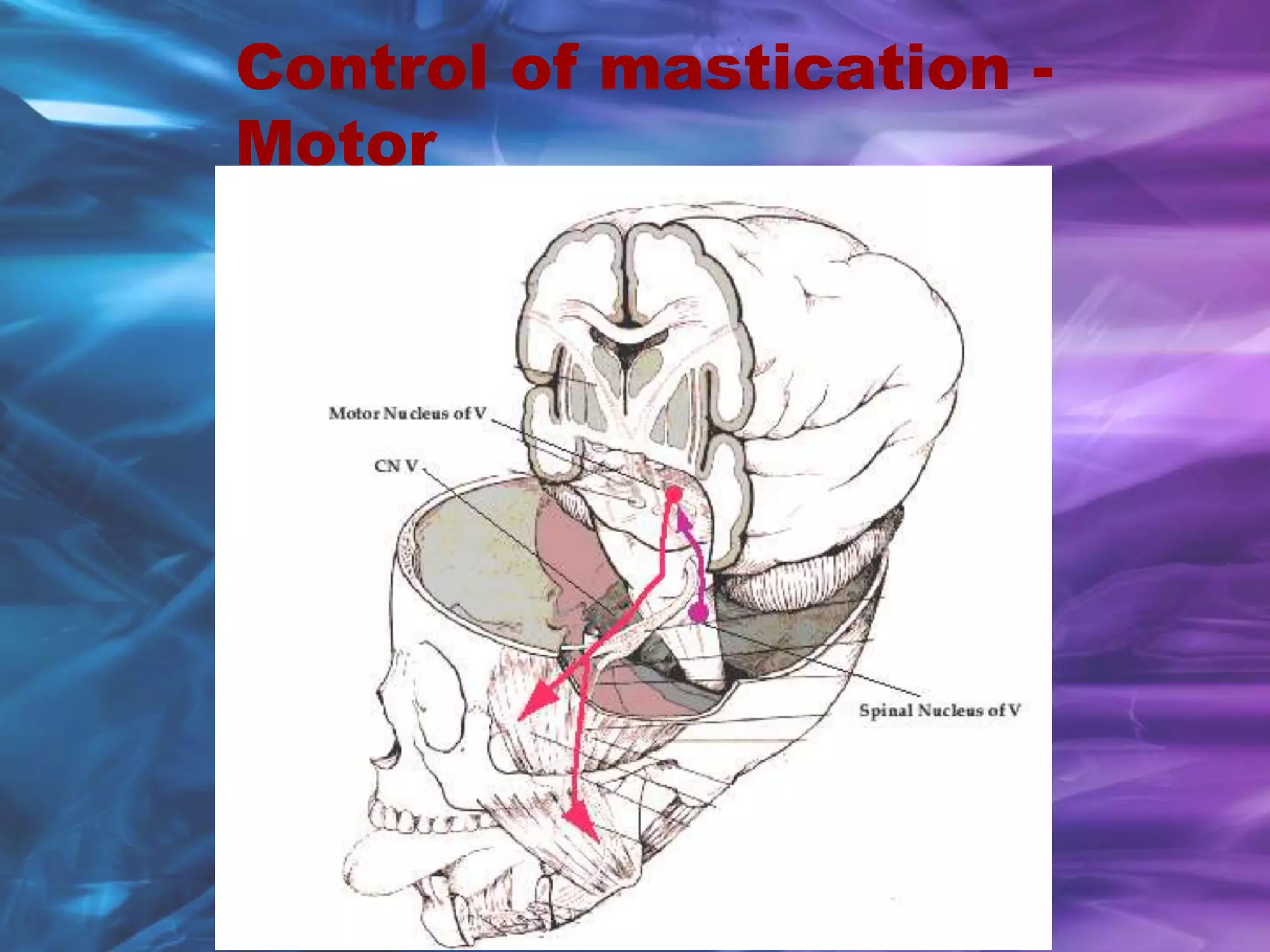
2) The muscles of mastication work in a coordinated manner through opening and closing strokes to crush and grind food between the teeth. Sensory feedback and reflexes help coordinate this chewing cycle.
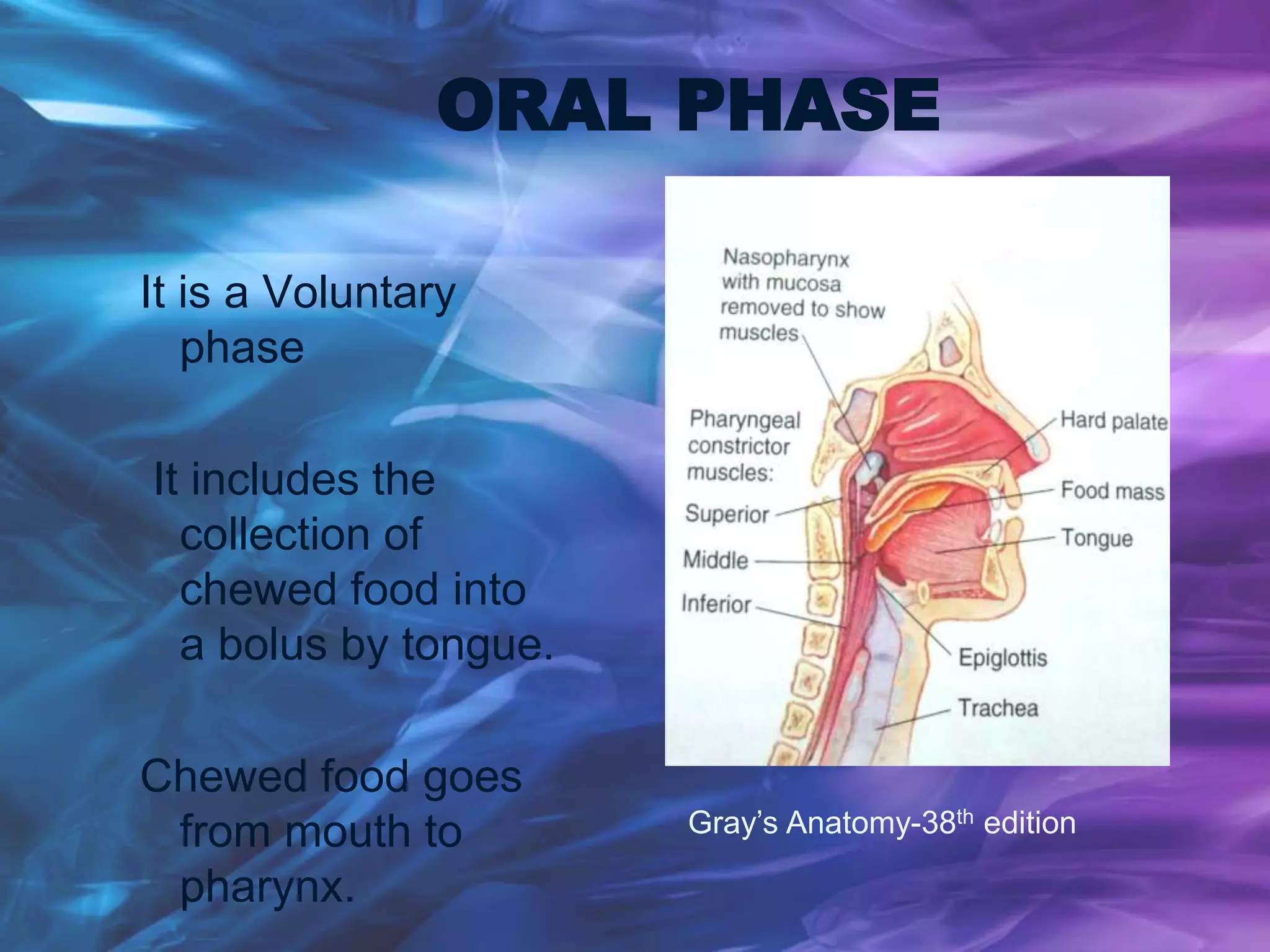
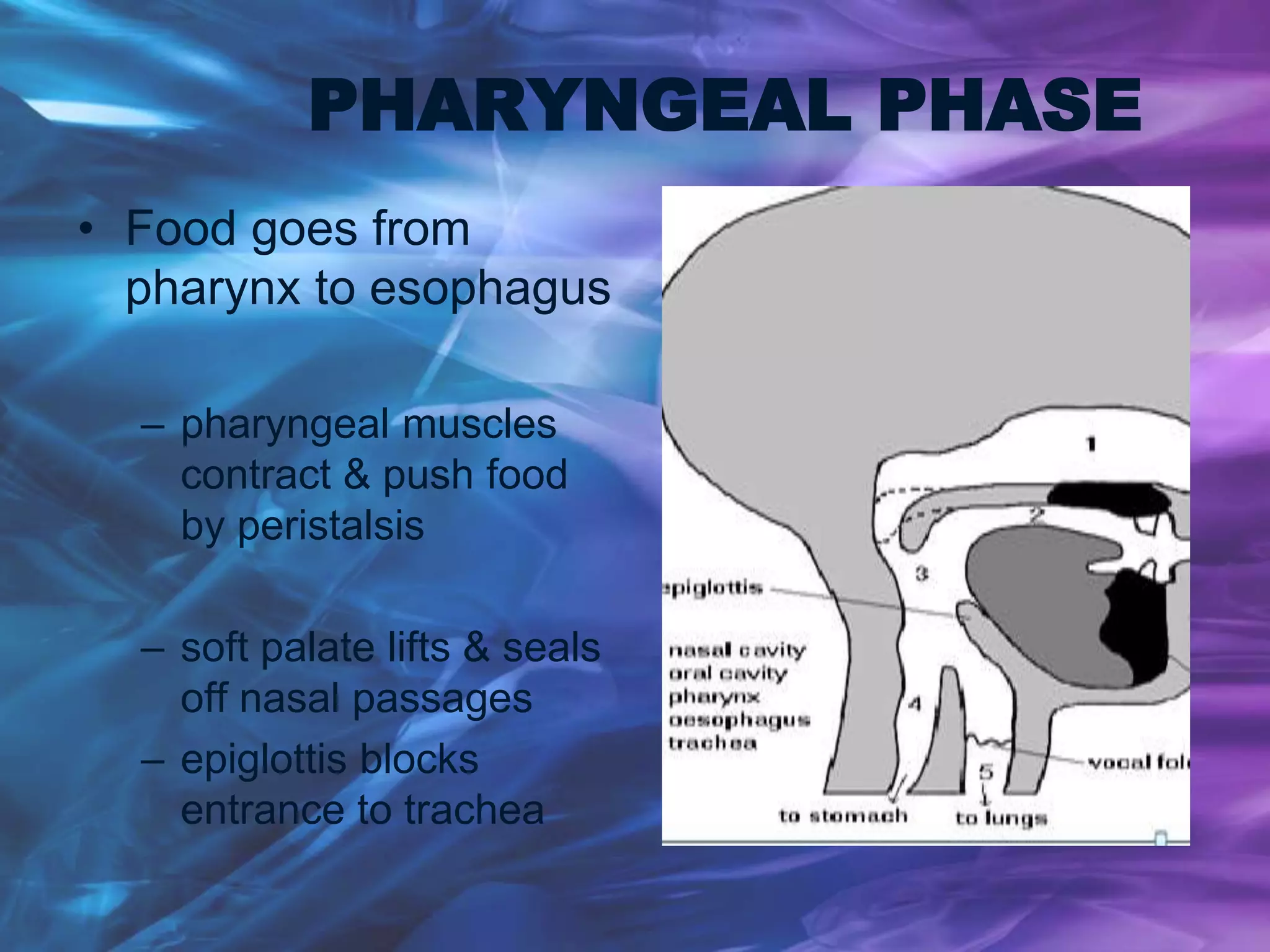
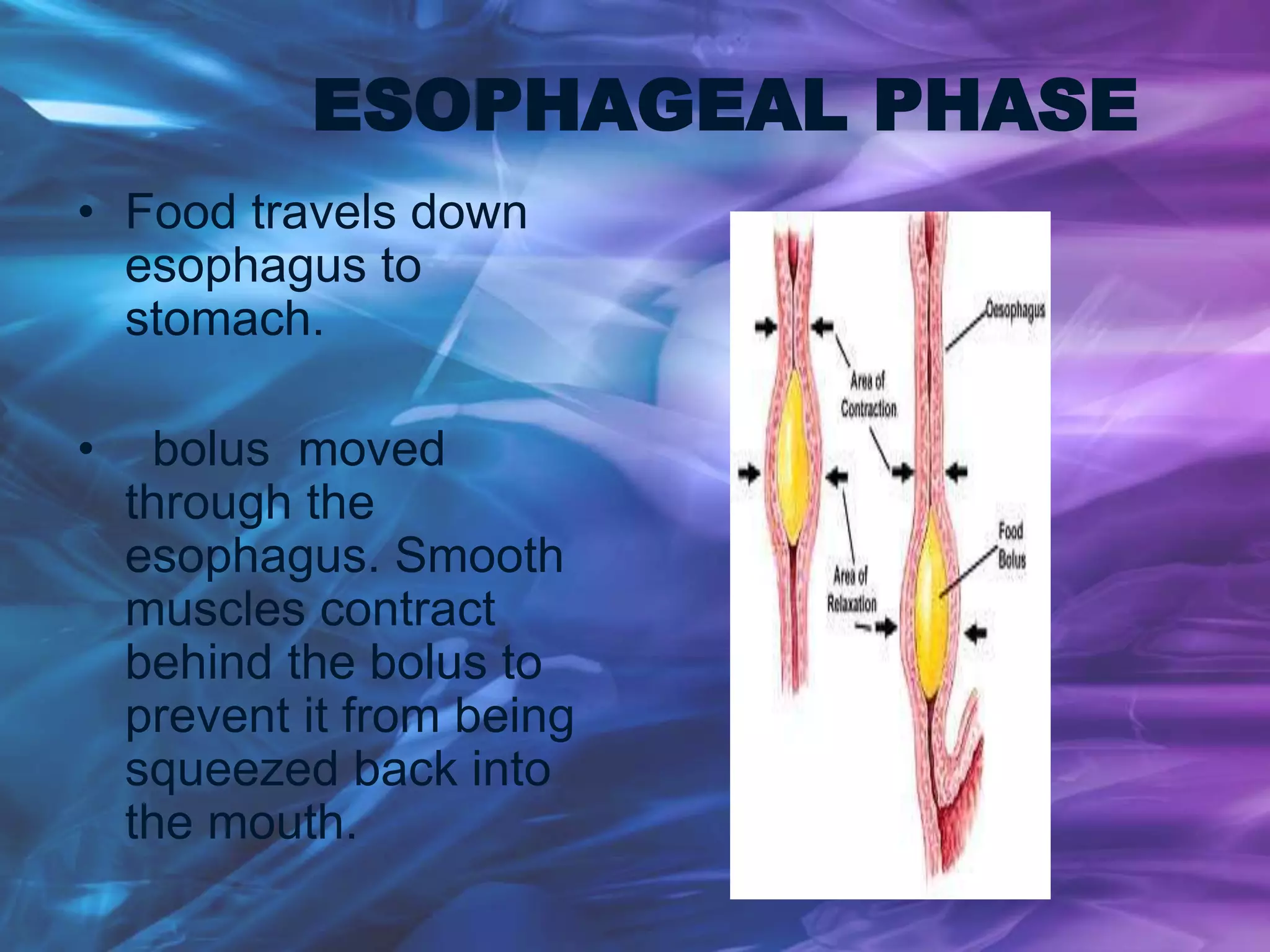
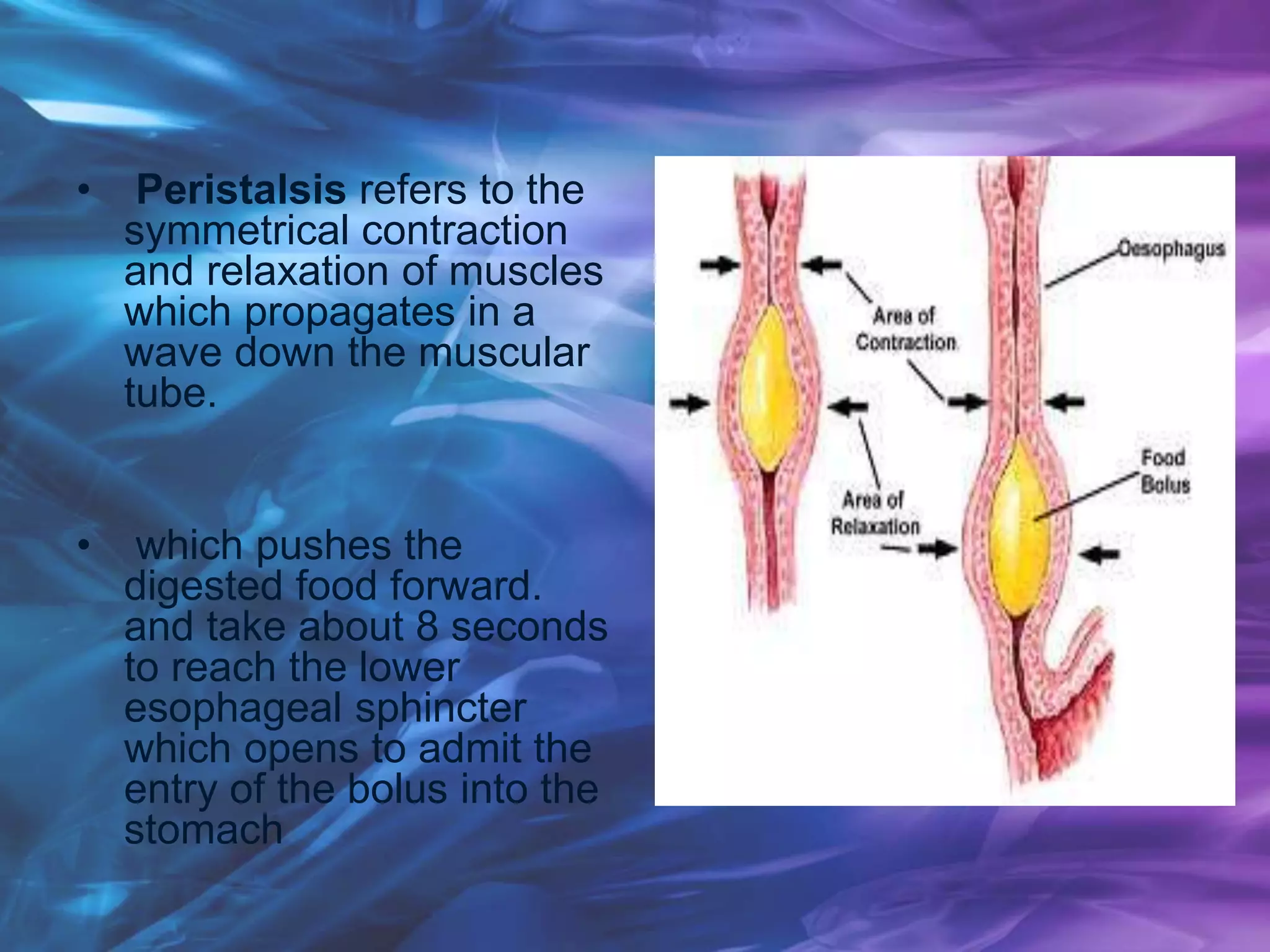
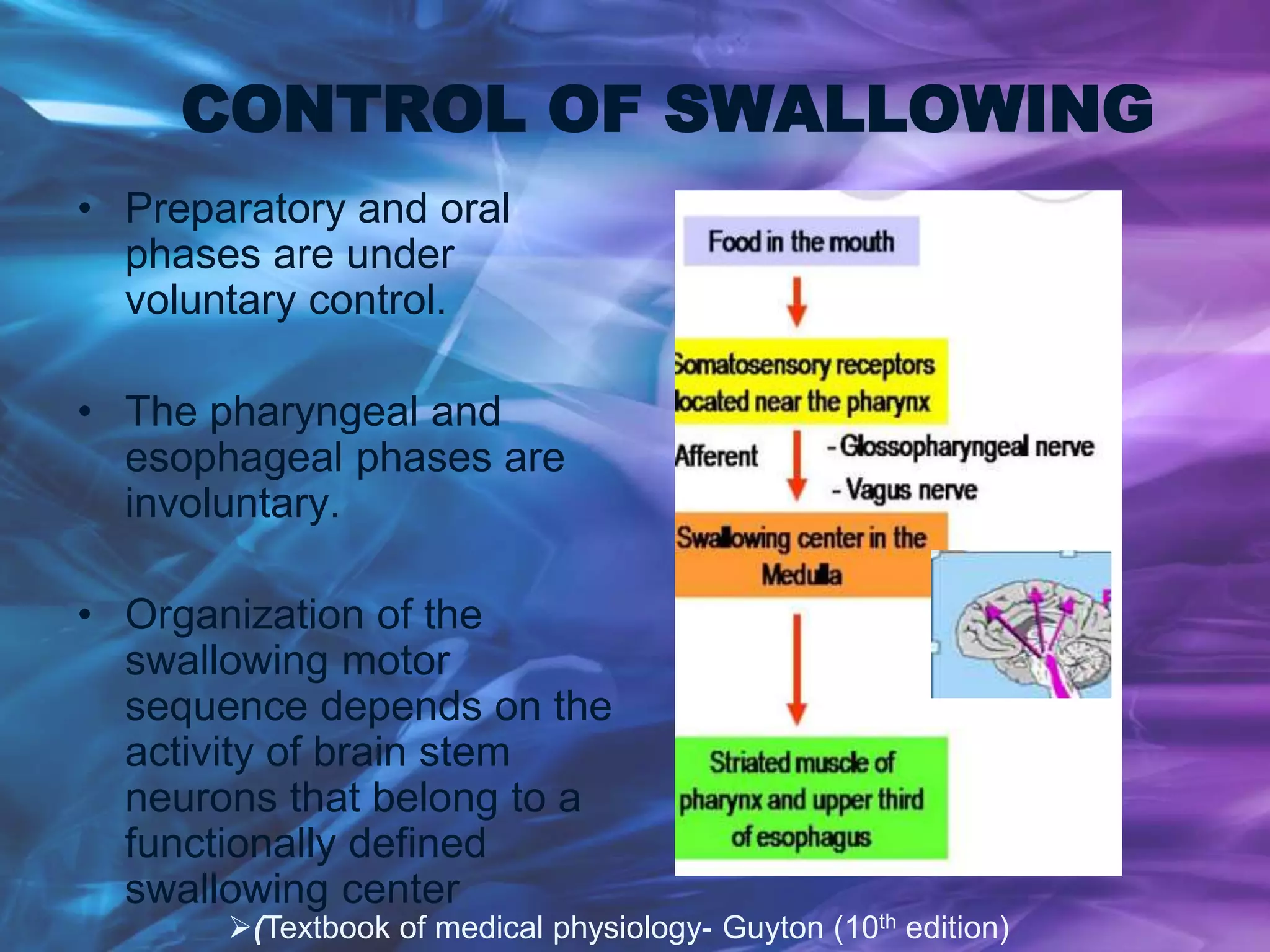
3) After sufficient mastication, the food is swallowed through a coordinated process of deglutition involving the oral, pharyngeal, and esophageal phases to transport the food bolus to the stomach for further digestion.
























![Anatomical landmarks of maxilla and mandible [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/anatomicallandmarksofmaxillaandmandibleautosaved-200820132830-thumbnail.jpg?width=640&height=640&fit=bounds)











![seminar 3 - physiology of MASTICATION AND DEGLUTITION [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/seminar3-physiologyofmasticationanddeglutitionautosaved-241029023716-692a8868-thumbnail.jpg?width=640&height=640&fit=bounds)




































