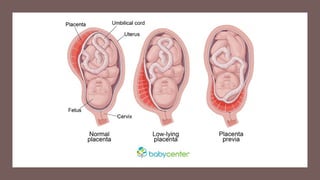
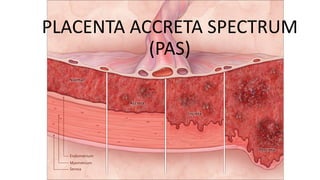
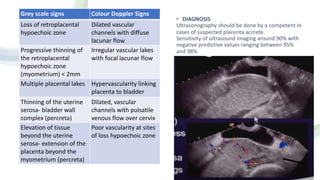
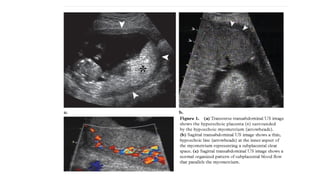
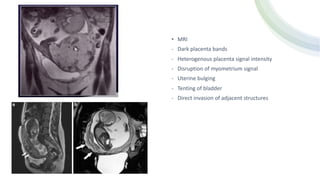
This document discusses placenta previa and placenta accreta spectrum. It begins with definitions of placenta previa as implantation of the placenta over the internal cervical os. It describes placenta accreta spectrum from accreta where the placenta attaches to the myometrium without decidua, to increta with invasion into the myometrium, and percreta with invasion through the myometrium. Risk factors include placenta previa, cesarean sections, advanced maternal age, and previous uterine surgeries. Ultrasound is the main diagnostic tool but MRI can also be used. Management involves multidisciplinary care, conservative approaches when possible