Download to read offline
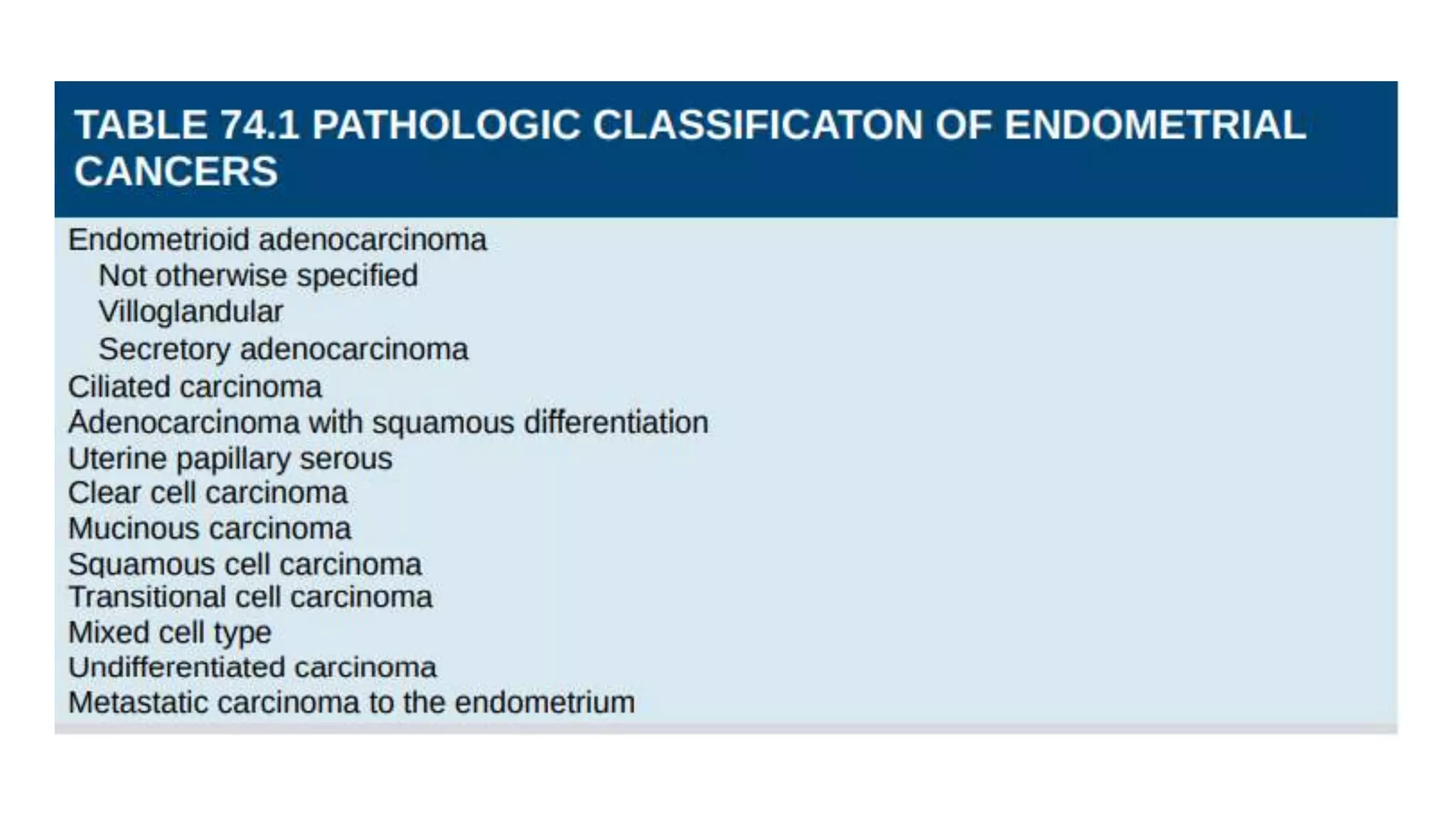
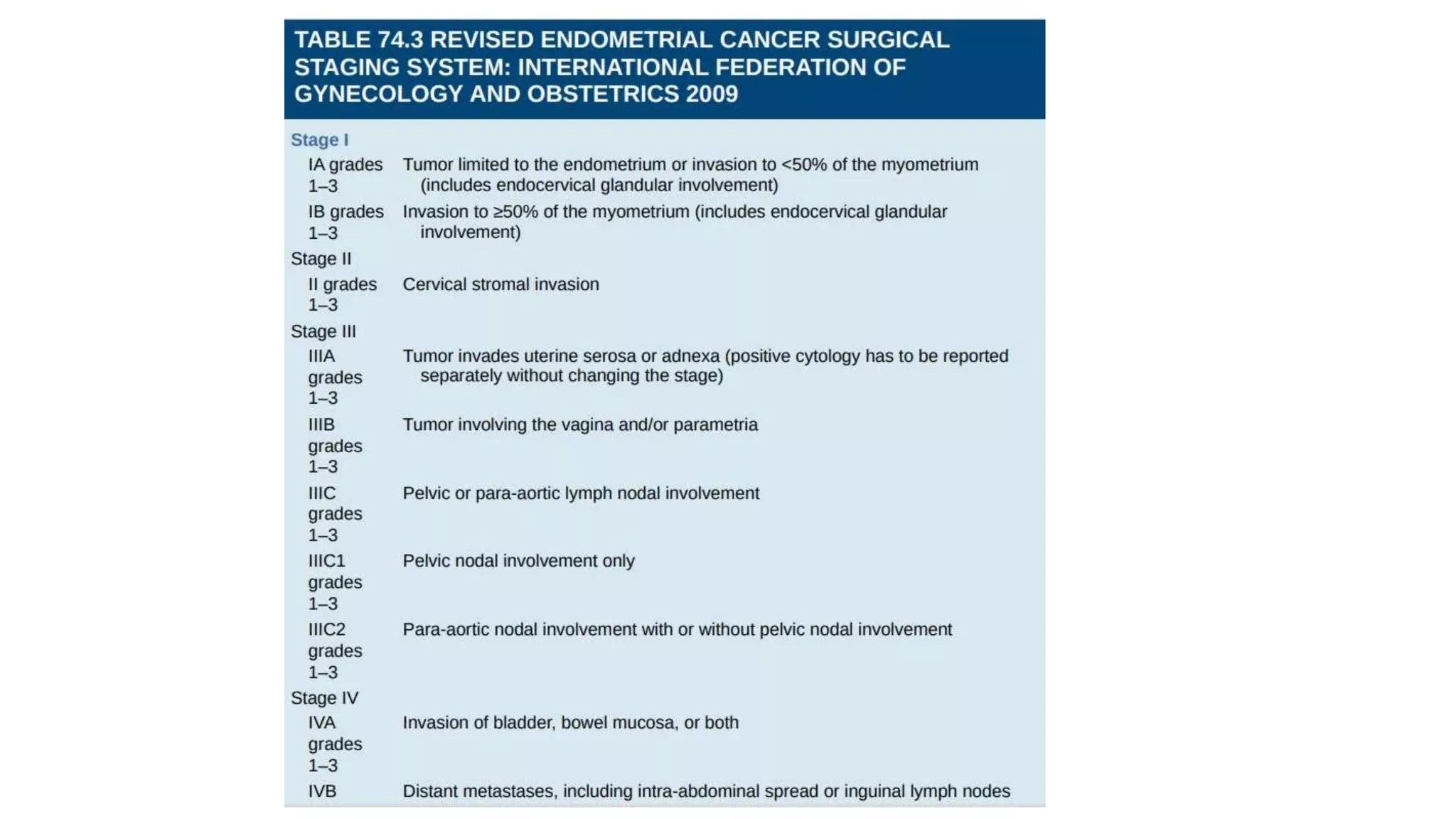
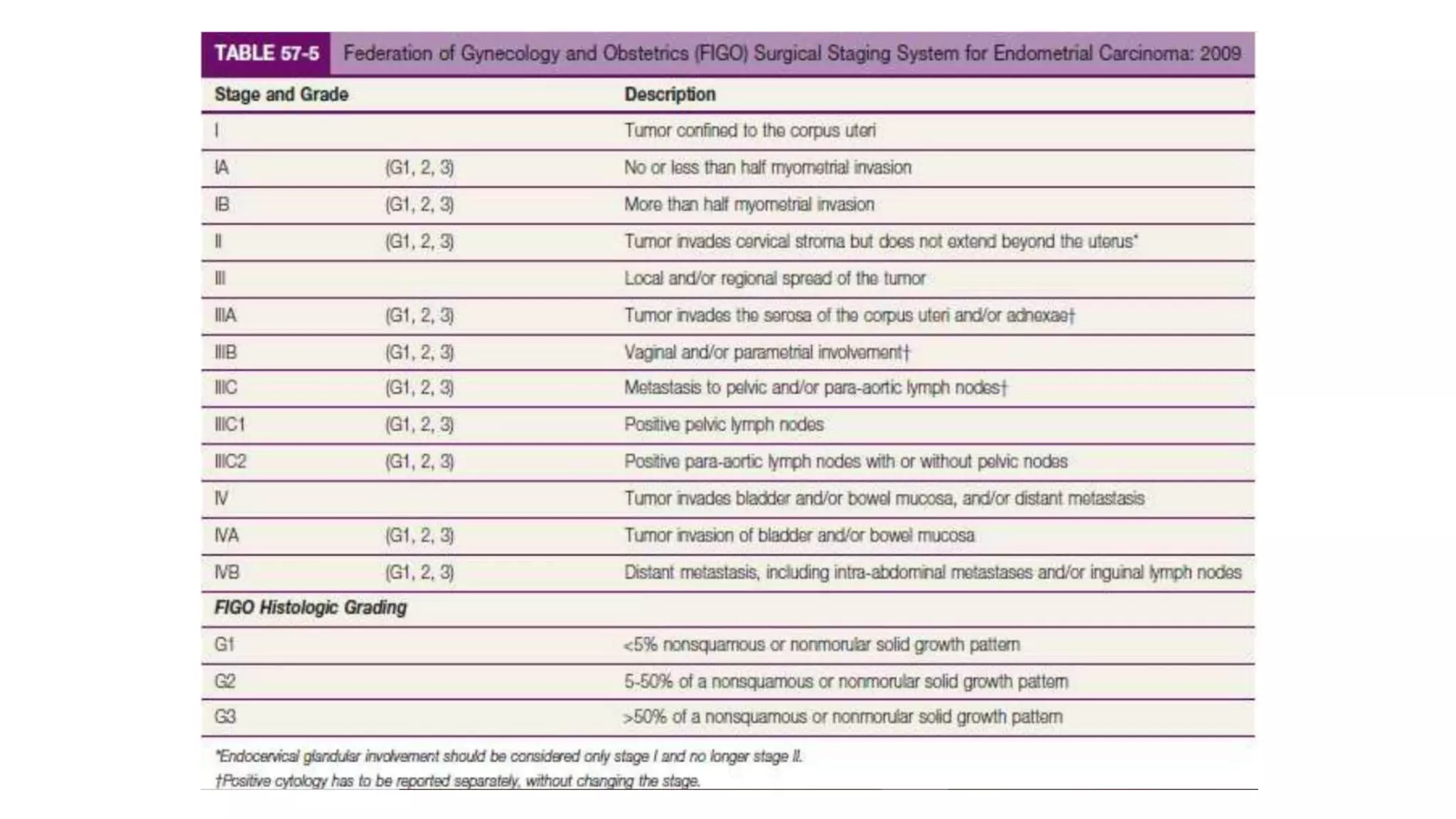
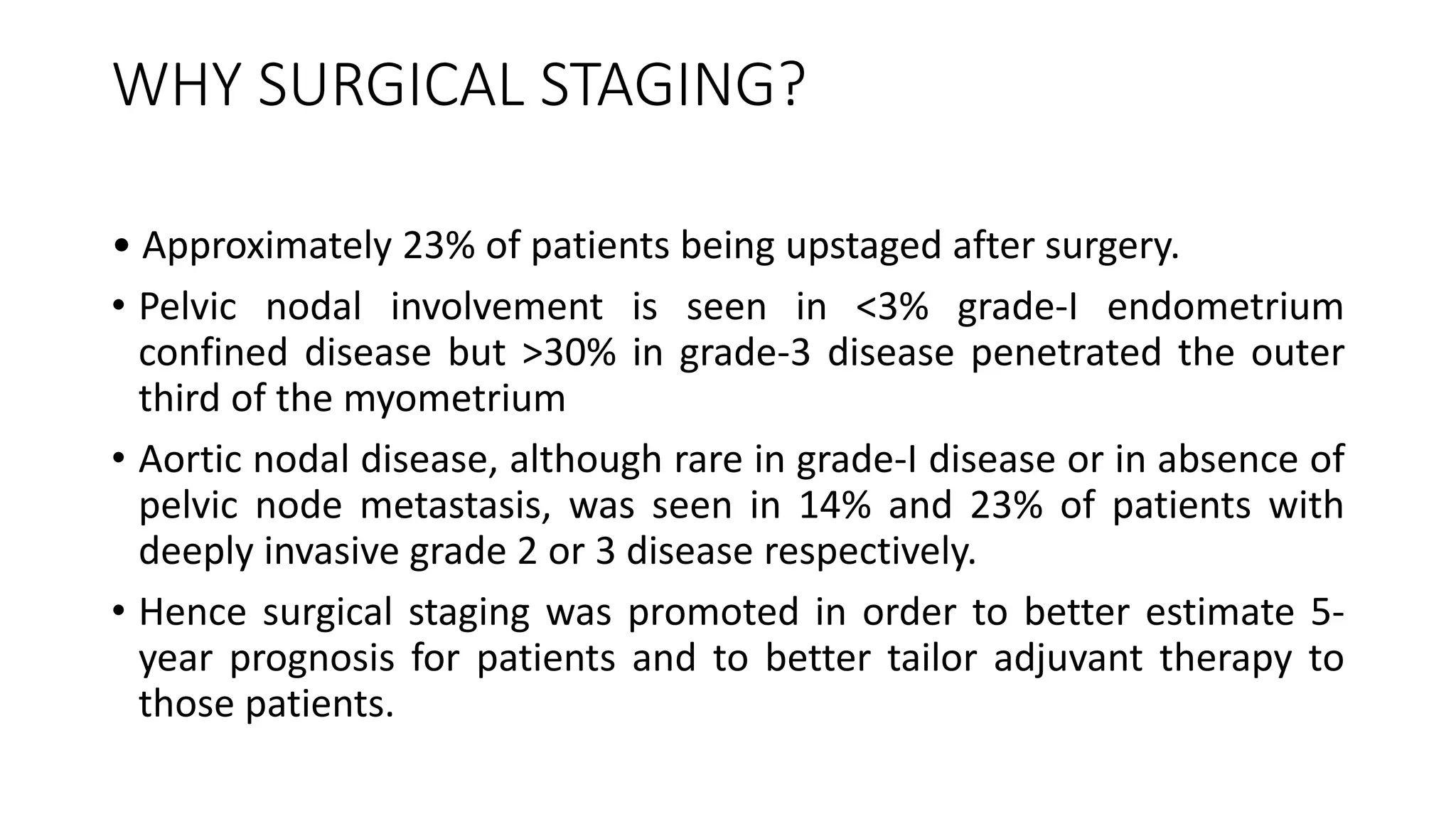
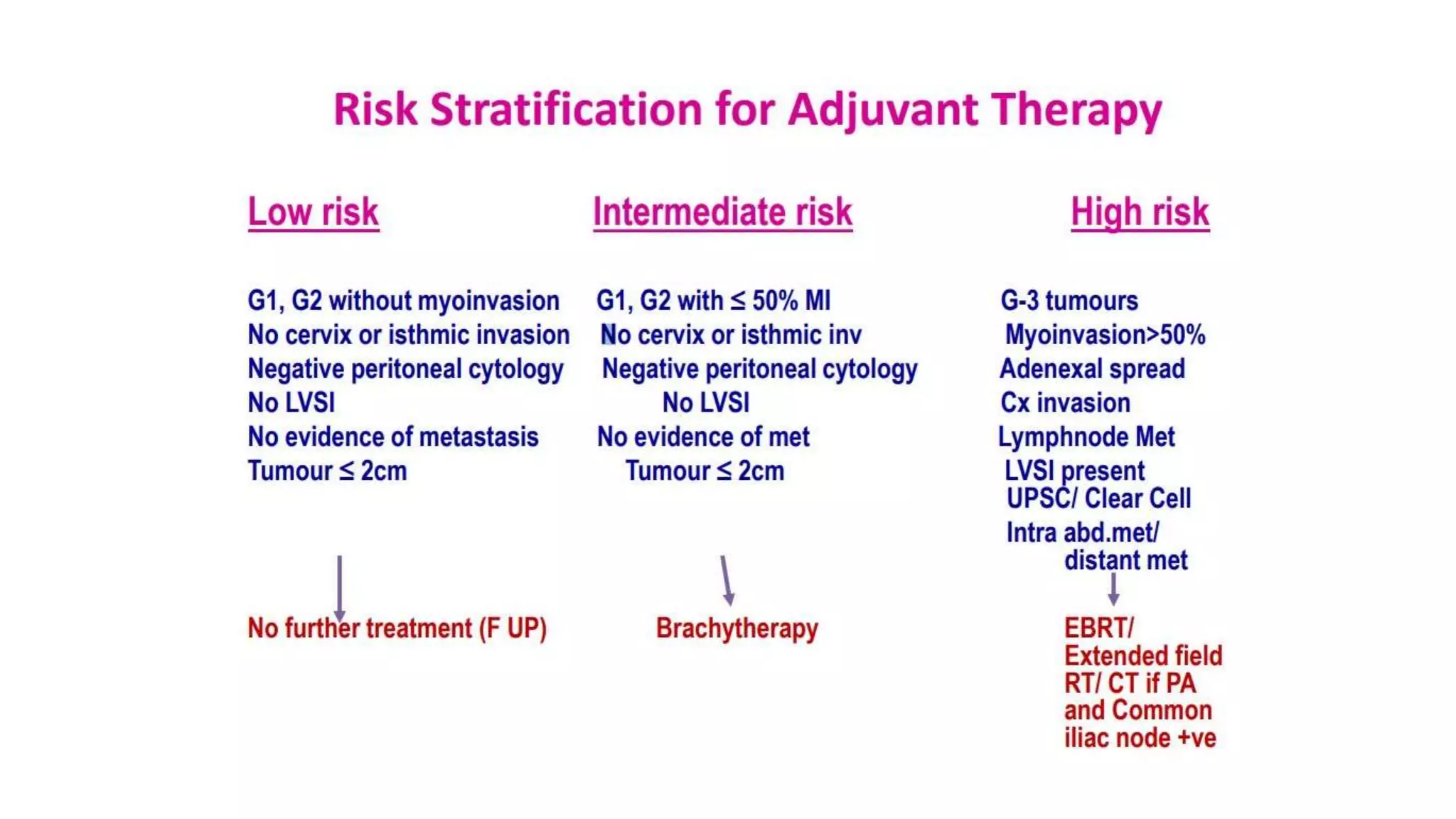
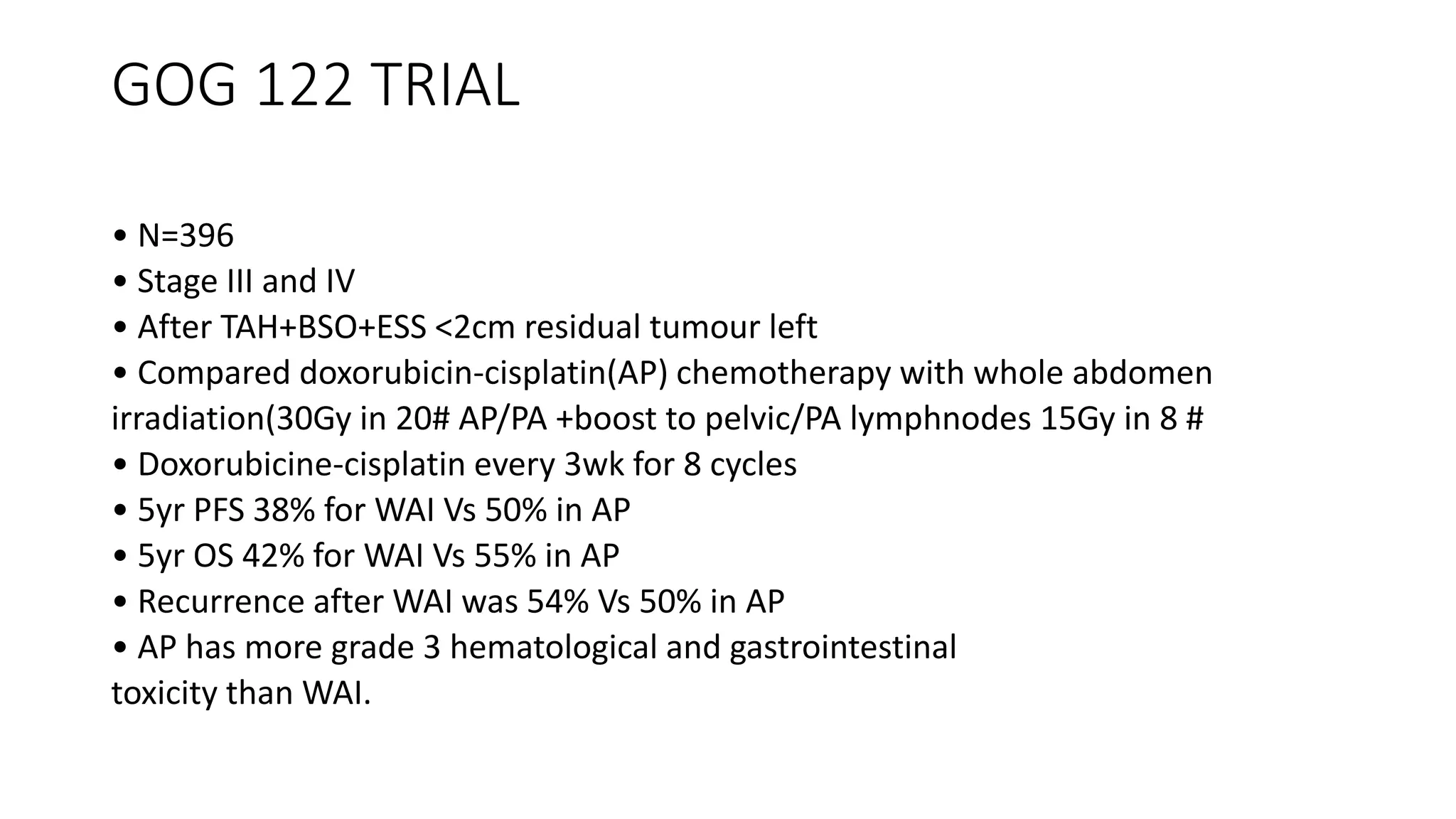
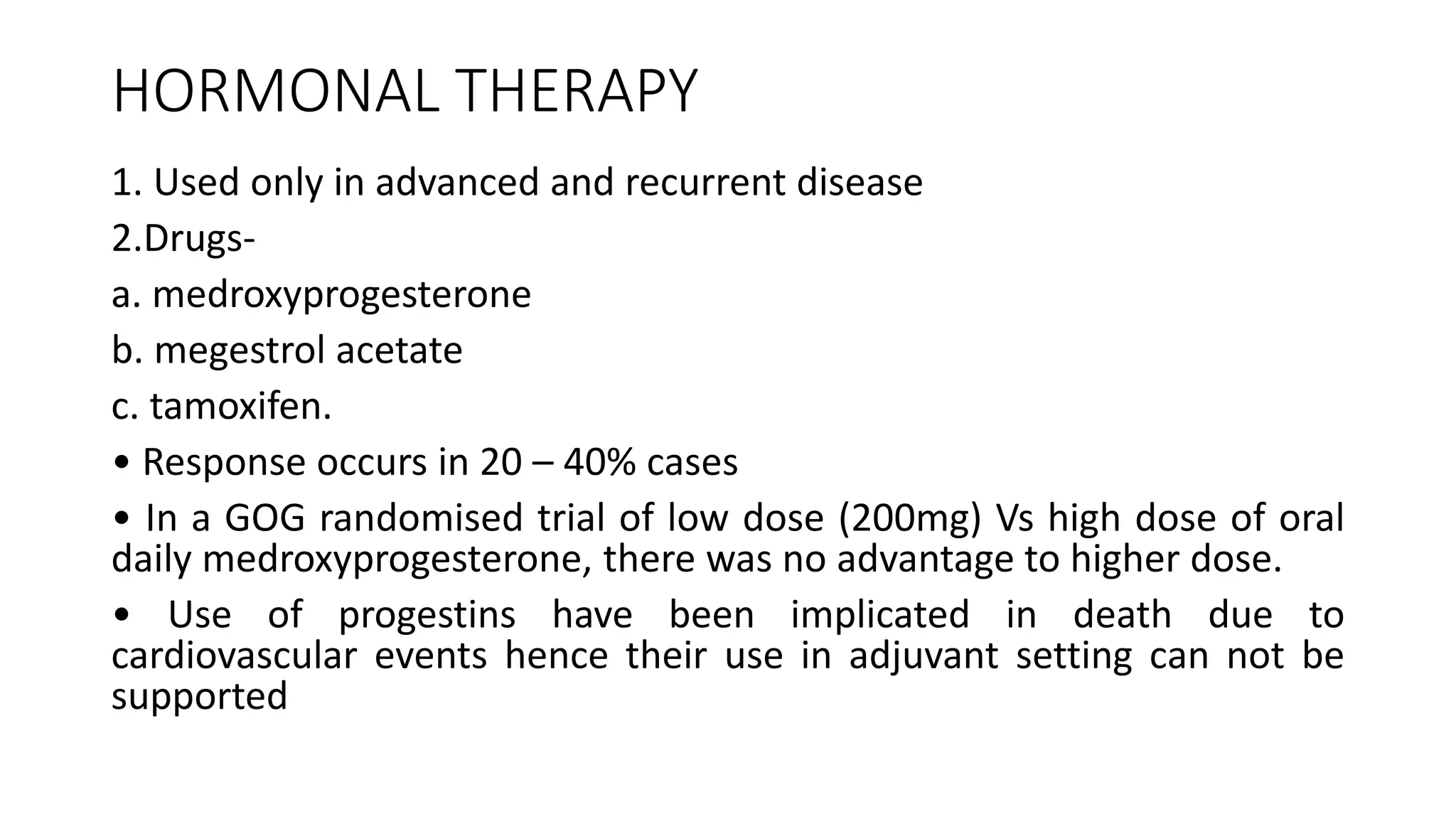
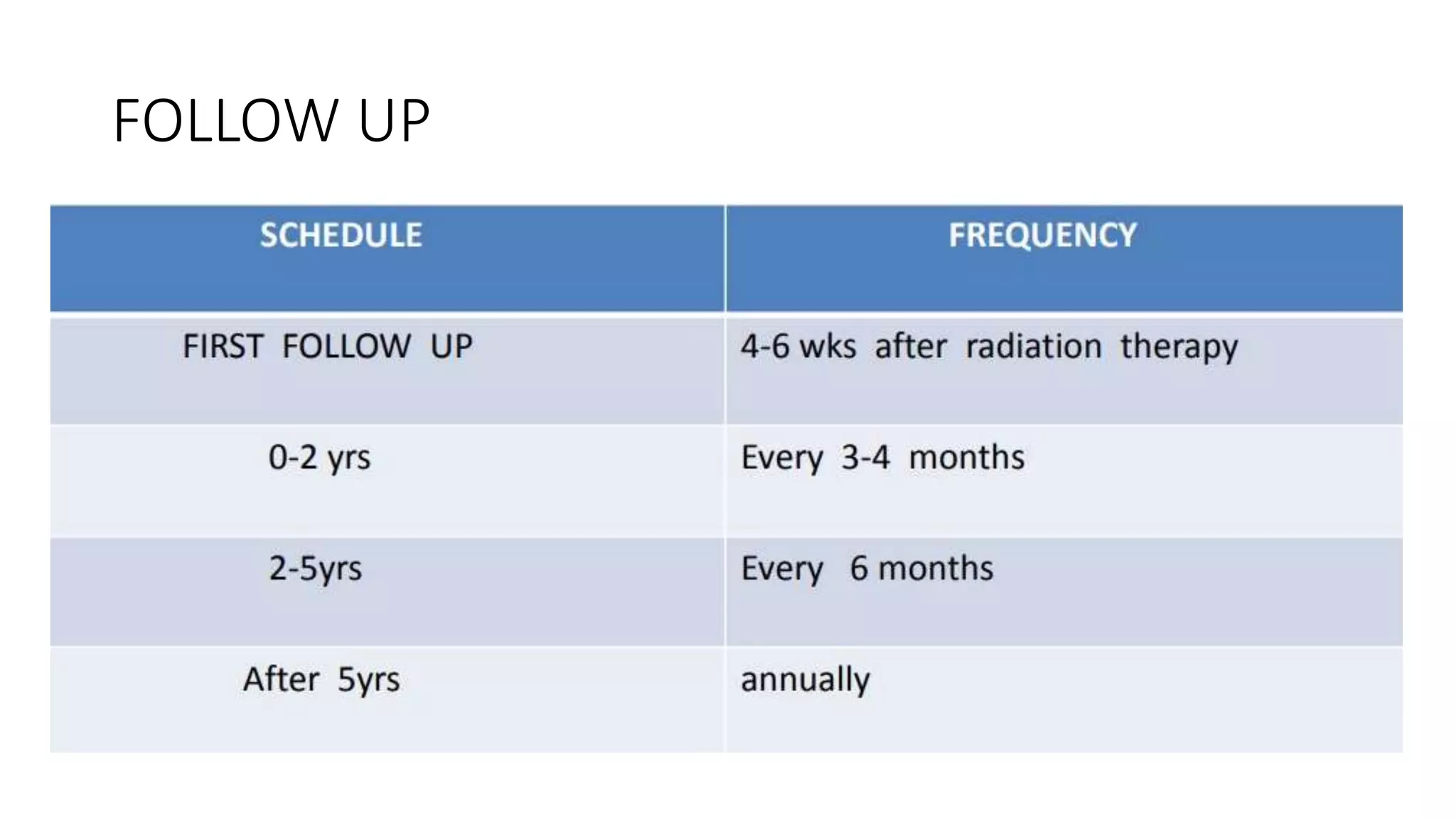
The document discusses the management of carcinoma endometrium, which includes diagnosis, staging, treatment, and follow up. Key points include: surgical staging is now standard to accurately identify disease extent and guide adjuvant therapy; total abdominal hysterectomy and bilateral salpingo-oophorectomy with surgical staging is the primary treatment for early stage disease; adjuvant radiation therapy, chemotherapy, or hormonal therapy may be used depending on risk factors like grade, myometrial invasion, and lymphovascular space invasion status. Randomized controlled trials have established the benefit of doxorubicin and cisplatin chemotherapy over whole abdominal radiation for advanced stage disease. Prognostic factors, treatment recommendations, and follow up considerations are also outlined.



































































