Downloaded 322 times











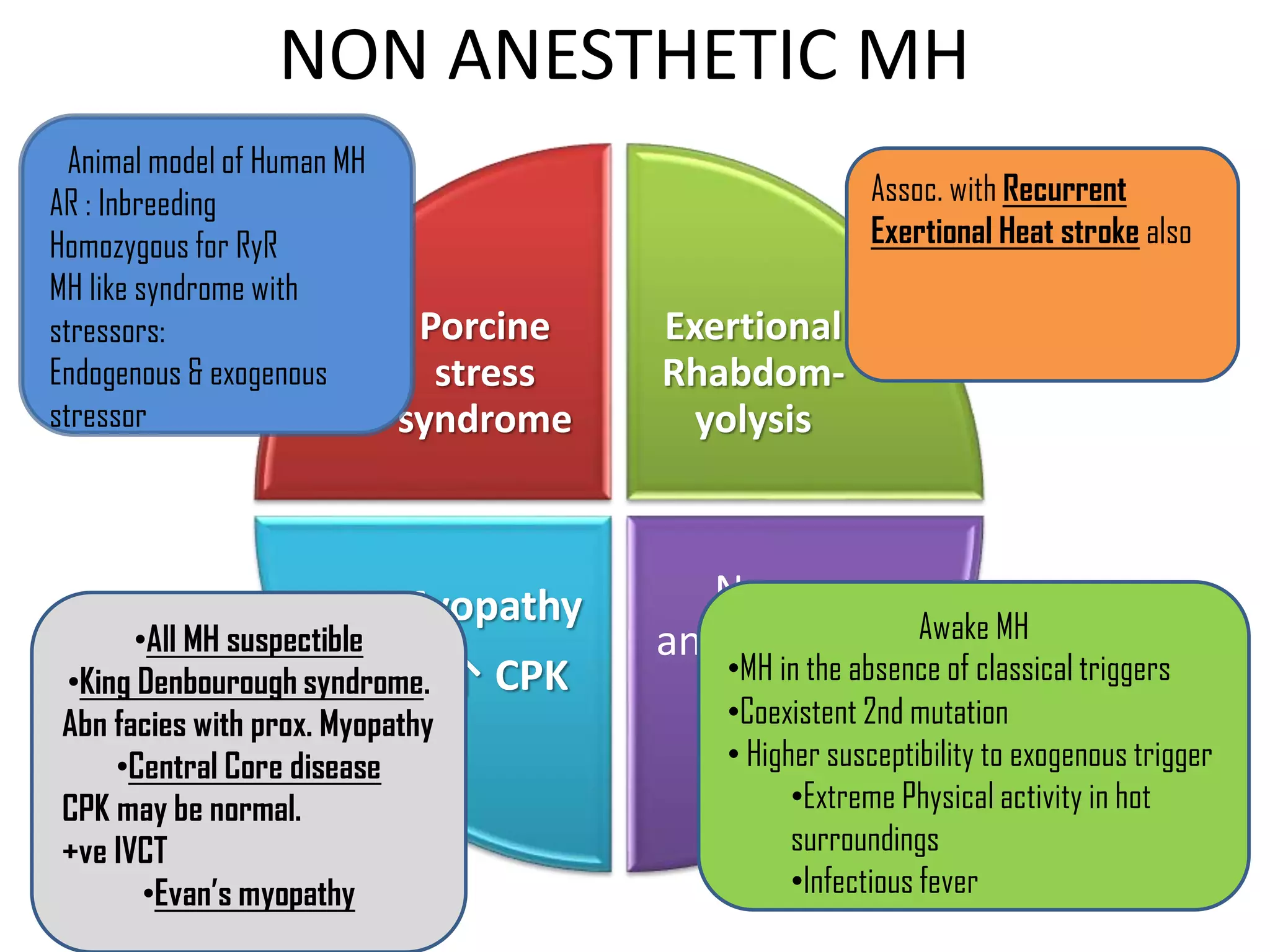
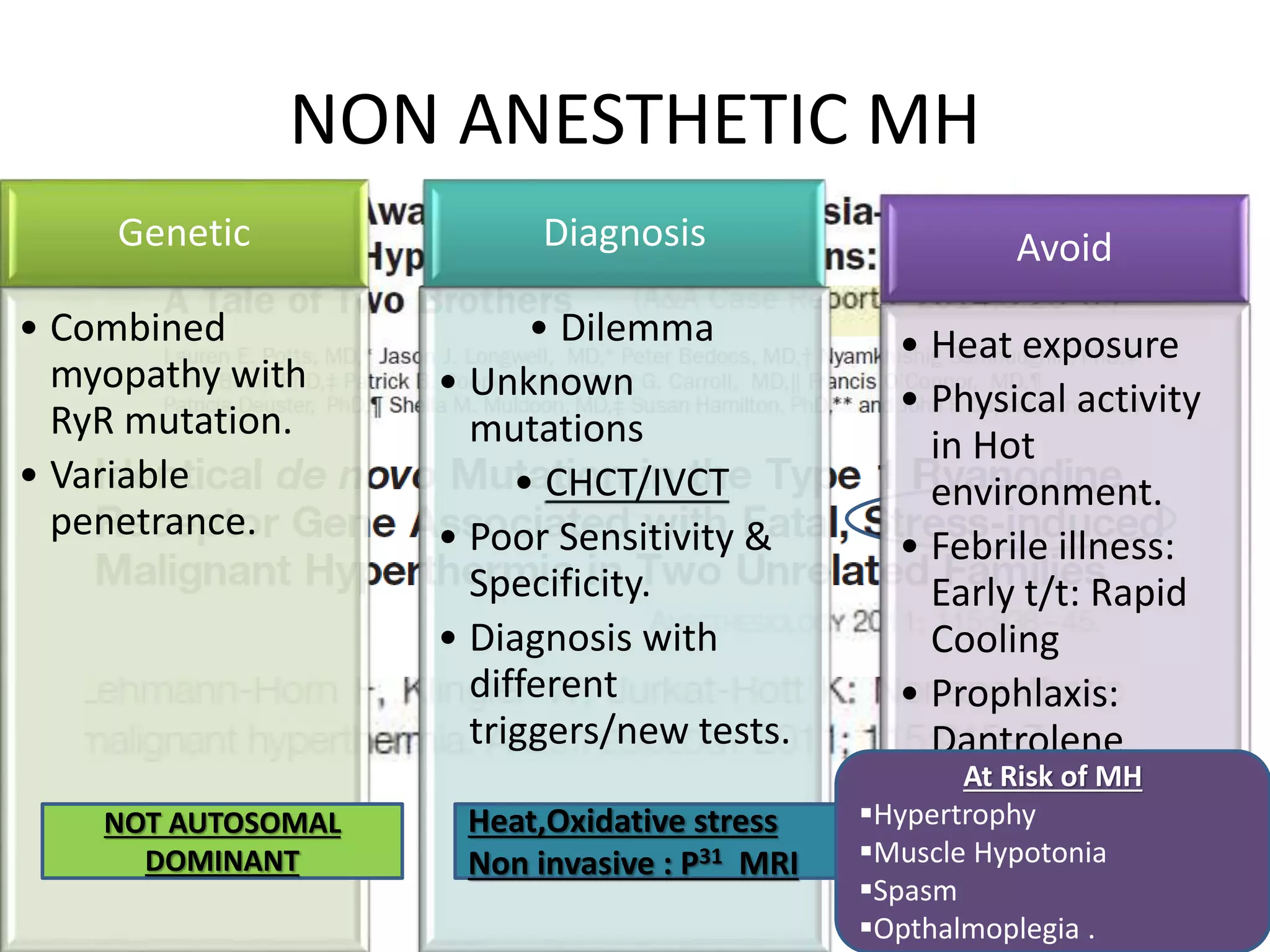







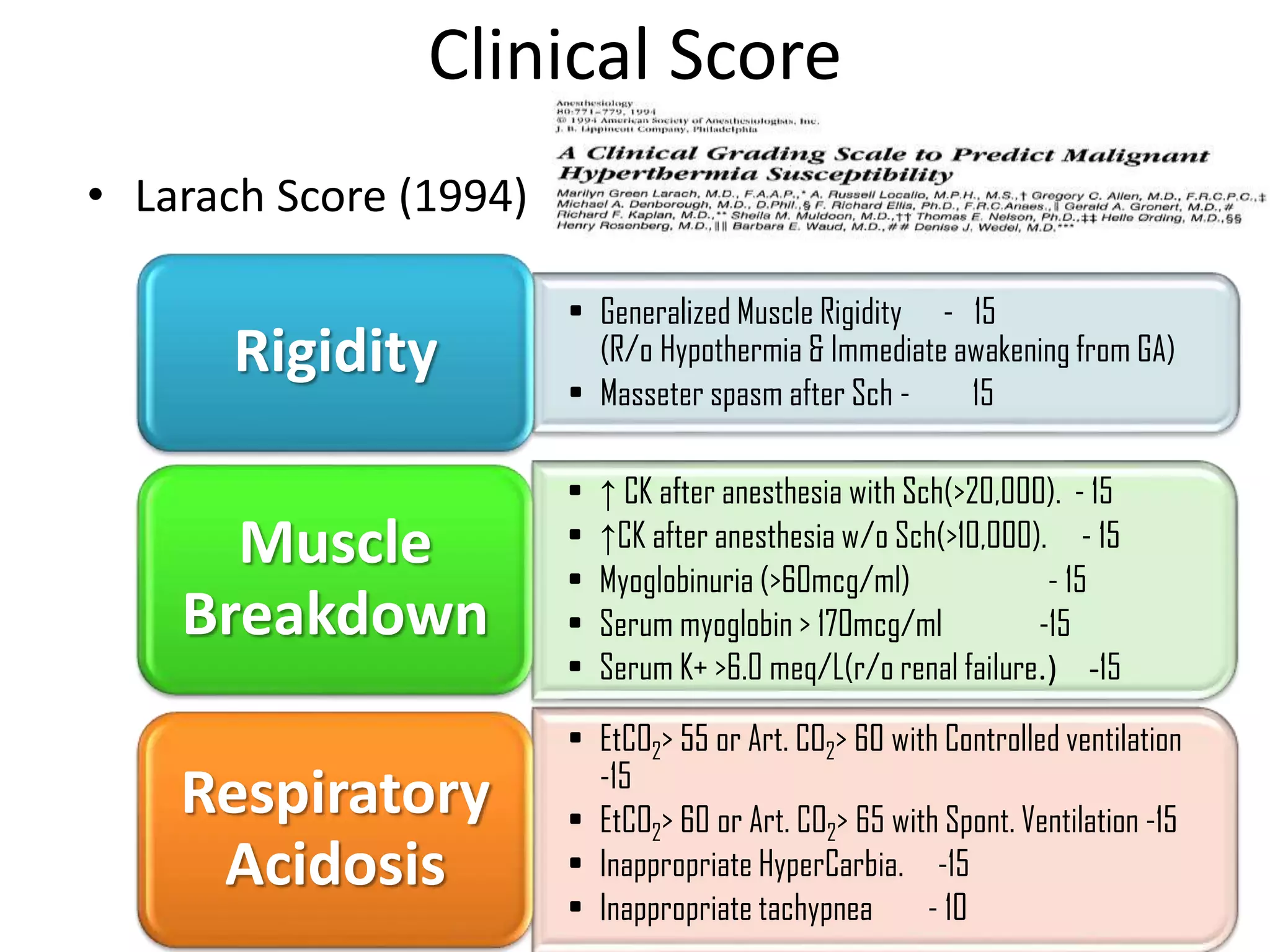





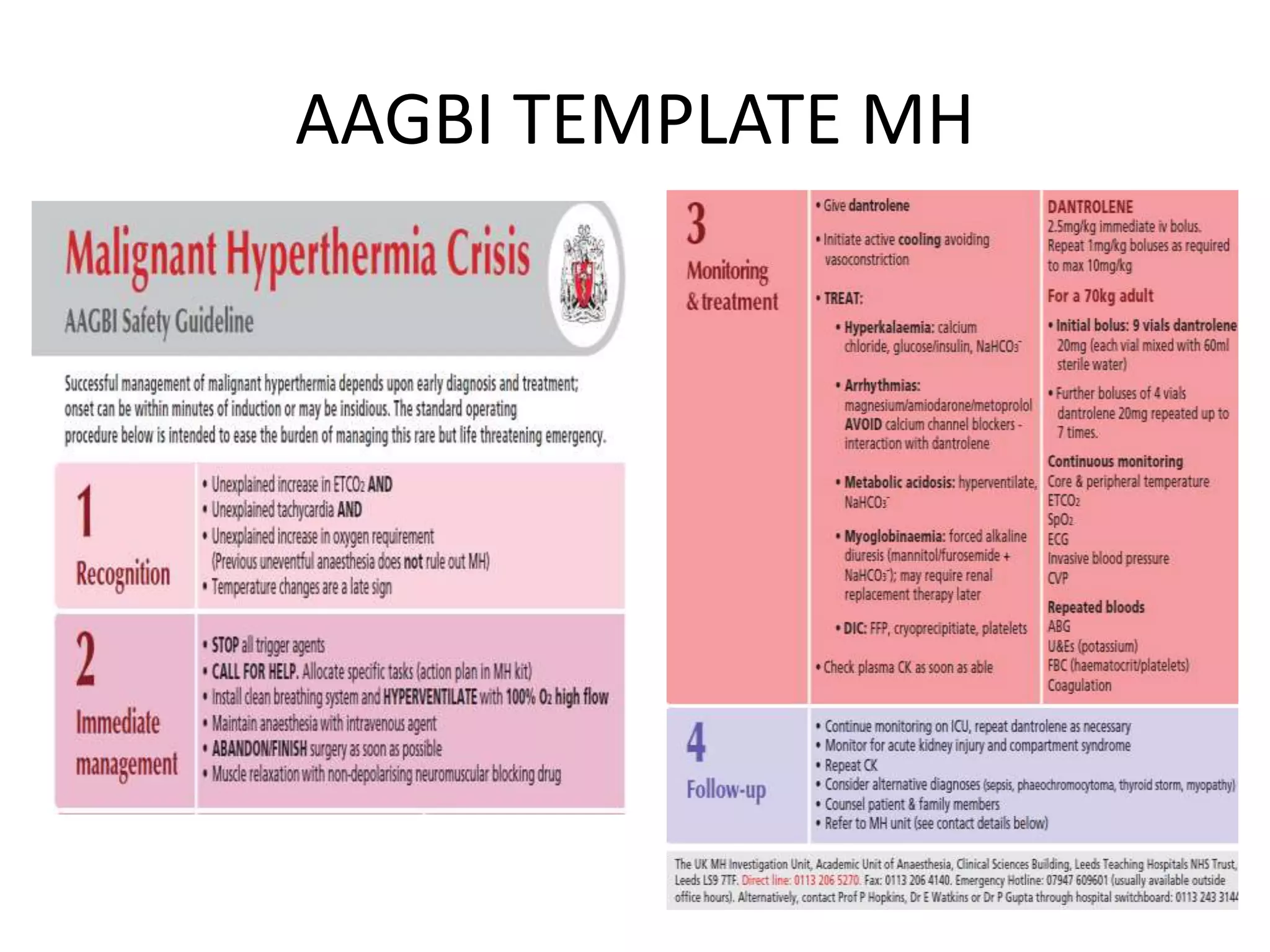








Malignant hyperthermia is a pharmacogenetic disorder triggered by volatile anesthetic gases and succinylcholine. It results in an abnormal rise in intracellular calcium in genetically susceptible individuals which leads to rapid increases in body temperature, muscle rigidity, and metabolic acidosis that can be fatal if not treated promptly. The key features of malignant hyperthermia include inappropriate tachycardia, arrhythmias, acidosis, hypercarbia, muscle breakdown and a rapid rise in temperature. Treatment involves immediately terminating the triggering agents, active cooling, hyperventilation with 100% oxygen, administration of dantrolene to reduce calcium levels in the muscle, and treating complications like acidosis and hyperkalemia