Malignant hyperthermiais a pharmacogenetic disorder inherited primarily
in an autosomal dominant pattern
It is a rare [1:15000 (paediatric) & 1:40,000 (adult)] genetic hypermetabolic
state
The earlier an episode of MH identified and treated –better the outcome.
Men> Women
3.
GENETIC FACTOR
Genefor the Ryanodine (Ryr1) receptor located on chromosome 19
Ryr1 is a calcium channel responsible for Ca2+ release from
sarcoplasmic reticulum & it play an important role in muscle
depolarization and closely associated dihydropyridine (DHP).
Mutation in MH
Uncontrolled release or increase in intracellular calcium in skeletal
muscle from sarcoplasmic reticulum .
Loss of inhibition of troponin..
Sustained muscle contraction.
Markedly increased ATP.
Uncontrolled hypermetabolic state.
Increased oxygen consumption .
Severe lactic acidosis
Hyperthermia
CLINICAL FEATURES
Timingof presentation :-
Highly variable
The initial sign of MH may occur soon after induction with general
anaesthetic agent (volatile agent or succinylcholine )
OR
Any time during the maintenance phase of anaesthesia.
7.
Sequence ofclinical sign :-
Unexplained and unexpected increased in ETCO2 .
Unexplained and unexpected increased in heart rate .
Tachypnea if spontaneous ventilation present .
Unexplained decreased in O2 saturation .
Unexplained and unexpected increase in body temperature ( above 38.8
) .
℃
Unexpected metabolic and respiratory acidosis .
More then one signs of the above should be present to make the diagnosis
of MH.
8.
CLINICAL MANIFESTATION
INCREASED METABOLISM
Increased co2 production (An unanticipated doubling and tripling of ETCO2
early and sensitive indicator)
Increased O2 consumption
Decreased mixed venous oxygen tension
Metabolic acidosis
Cyanosis
Mottling
INCREASED SYMPATHETIC ACTIVITY
Tachycardia
Hypertension f/b hypotension
Arrhythmia
Stage 1:- Sustainedmuscle contraction [ masseter spasm ,sinus tachycardia ]
High metabolic level [ increased O2 and glucose consumption , increased CO2 ,lactic
acid and heat production ]
Stage 2 :-Progression stage
Hypercarbia ( respiratory acidosis ) tachycardia and some cases visible muscle rigidity
occurs
Switching to anaerobic metabolism can worsen acidosis due to the production of
lactic acid ,resulting in mixed respiratory and metabolic acidosis
Once energy ( ATP ) store are depleted ,rhabdomyolysis occur and result in
hyperkalaemia and myoglobinuria [ increased CK , Renal failure ]
Stage 3:-last stage
In this stage ,core body temperature rise by as much as 1 degree Celsius every few
minutes .
Accelerated hyperthermia ( above 41degree Celsius ) is associated with a marked
increase in C02 production and increased oxygen consumption and can cause
widespread vital organ dysfunction and disseminated intravascular coagulation .
11.
CONDITIONS AND DISORDERSTHAT MAY
MIMIC MALIGNANT HYPERTHERMIA
Anaphylactic reaction
Alcohol therapy for limb arteriovenous malformation
Contrast dye injection
Hyperkalaemia
Diabetic coma
Drug toxicity or abuse
Elevated end-tidal CO2 due to laparoscopic operation
Environmental heat gain more than loss
Equipment malfunction with increased carbon dioxide
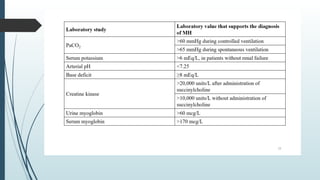
LABORATORY TESTING
Send bloodfor :-
ABG –repeated ( Approx every 30 minute )
CBC
SERUM ELECTROLYTE
SERUM CK
COAGULATION SCREEN
CROSS MATCH
Send urine for :- MYOGLOBIN
15.
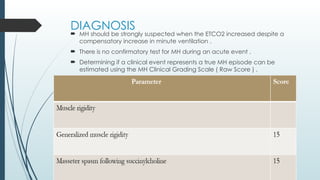
DIAGNOSIS
MH shouldbe strongly suspected when the ETCO2 increased despite a
compensatory increase in minute ventilation .
There is no confirmatory test for MH during an acute event .
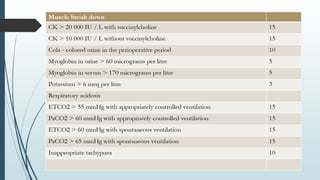
Determining if a clinical event represents a true MH episode can be
estimated using the MH Clinical Grading Scale ( Raw Score ) .
DIAGNOSIS IN SUSPECTEDINDIVIDUAL
Gold Standard: In-Vitro Caffeine Test(IVCT) and Caffeine Halothane
Contracture Test(CHCT)
IVCT: done by performing a muscle biopsy and exposing the muscle to
Caffeine and Halothane.
CHCT: muscle biopsy is done and exposed to increasing concentrations of
Halothane and response noted.
Preferred muscle: Vastus group and rectus abdominis
20.
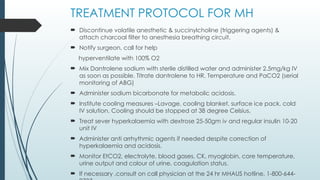
TREATMENT PROTOCOL FORMH
Discontinue volatile anesthetic & succinylcholine (triggering agents) &
attach charcoal filter to anesthesia breathing circuit.
Notify surgeon, call for help
hyperventilate with 100% O2
Mix Dantrolene sodium with sterile distilled water and administer 2.5mg/kg IV
as soon as possible. Titrate dantrolene to HR, Temperature and PaCO2 (serial
monitoring of ABG)
Administer sodium bicarbonate for metabolic acidosis.
Institute cooling measures –Lavage, cooling blanket, surface ice pack, cold
IV solution. Cooling should be stopped at 38 degree Celsius.
Treat sever hyperkalaemia with dextrose 25-50gm iv and regular insulin 10-20
unit IV
Administer anti arrhythmic agents if needed despite correction of
hyperkalaemia and acidosis.
Monitor EtCO2, electrolyte, blood gases, CK, myoglobin, core temperature,
urine output and colour of urine, coagulation status.
If necessary ,consult on call physician at the 24 hr MHAUS hotline, 1-800-644-
21.
DANTROLENE
Hydantoin derivative
Directly interfere with muscle contraction by binding to Ryr receptor and
inhibit calcium release from sarcoplasmic reticulum.
2.5mg/kg IV every 5 min until episode is terminated.
Effective half life 6 hour
To prevent relapse 1mg/kg IV every 6 hrs. for 24-48 hr.
Some cases of acute malignant hyperthermia may require 10-20 mg of
Dantrolene.
New formulation of Dantrolene (Ryenodex) require significantly less time for
reconstitution than older preparation.
22.
Dantrolene can bestopped, or the interval between doses increased to every
8 or 12 hours if all of the following criteria are met:
Metabolic stability for 24 hours
Core temp is less than 38°C
Creatine kinase (CK) is decreasing
No evidence of myoglobinuria
Muscle is no longer rigid
EVALUATION OF SUSCEPTIBILITY
Evaluation of susceptibility includes a history and physical examination to
detect any subclinical abnormality.
Blood CK values, when determined in a resting, fasting state without recent
trauma, reflect muscle membrane stability.
When the CK level is elevated in a close relative of a person with known
MHS, the relative may be considered to have MHS without contracture
testing.
Dantrolene must be avoided before biopsy because it masks the response
to contracture-producing drugs.
26.
After apatient is diagnosed as being MHS, DNA testing for mutations should
follow.
MHS patients and all patients who are not biopsy tested, but who present
with a clinical picture that suggests a high probability for MHS, should be
given advice.
Awake episodes are uncommon, and if not experienced before diagnosis,
they are an unlikely problem.
27.
ANAESTHESIA FOR SUSCEPTIBLE
INDIVIDUAL
Nitrous oxide, barbiturates, etomidate, propofol, opioids and NDMR are
safe for such individuals.
Potent volatile anesthetics and succinylcholine must be avoided, even in
the presence of dantrolene.
Regional anesthesia should be preferred.
A dedicated machine/workstation should be present for MH susceptible
patients.
Preoperative dantrolene is never needed.
28.
If thereis no dedicated machine for MHS patients, flushing the anesthesia
workstation to less than 5 parts per million (ppm) of the volatile anesthetic
agent concentration is generally accepted .
Any facility using MH triggers on an inpatient or outpatient basis should
have dantrolene available immediately .
29.
NONANAESTHETIC MALIGNANT
HYPERTHERMIA
MHcan be triggered by stress such as exercise and overheating, known as
“awake” MH.
RyR1 mutations found to be present in the patients with exercise-induced
rhabdomyolysis.
These responses are related to muscle movement or to increased
temperature.
Stresses associated with these episodes include exercise and environmental
exposure to volatile non -anesthetic vapours.

![ Malignant hyperthermia is a pharmacogenetic disorder inherited primarily
in an autosomal dominant pattern
It is a rare [1:15000 (paediatric) & 1:40,000 (adult)] genetic hypermetabolic
state
The earlier an episode of MH identified and treated –better the outcome.
Men> Women](https://image.slidesharecdn.com/malignanthyperthermia-250223134556-ad91a54b/85/MALIGNANT-HYPERTHERMIA-and-its-management-pptx-2-320.jpg)



![Stage 1:- Sustained muscle contraction [ masseter spasm ,sinus tachycardia ]
High metabolic level [ increased O2 and glucose consumption , increased CO2 ,lactic
acid and heat production ]
Stage 2 :-Progression stage
Hypercarbia ( respiratory acidosis ) tachycardia and some cases visible muscle rigidity
occurs
Switching to anaerobic metabolism can worsen acidosis due to the production of
lactic acid ,resulting in mixed respiratory and metabolic acidosis
Once energy ( ATP ) store are depleted ,rhabdomyolysis occur and result in
hyperkalaemia and myoglobinuria [ increased CK , Renal failure ]
Stage 3:-last stage
In this stage ,core body temperature rise by as much as 1 degree Celsius every few
minutes .
Accelerated hyperthermia ( above 41degree Celsius ) is associated with a marked
increase in C02 production and increased oxygen consumption and can cause
widespread vital organ dysfunction and disseminated intravascular coagulation .](https://image.slidesharecdn.com/malignanthyperthermia-250223134556-ad91a54b/85/MALIGNANT-HYPERTHERMIA-and-its-management-pptx-10-320.jpg)














![Malignant hyperthermia [final]](https://cdn.slidesharecdn.com/ss_thumbnails/malignanthyperthermiafinal-160608094814-thumbnail.jpg?width=640&height=640&fit=bounds)














































