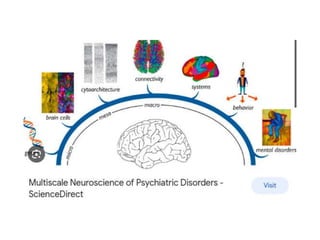
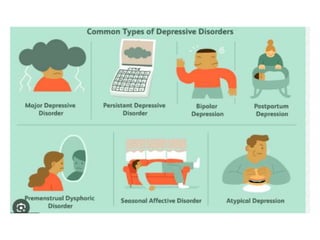
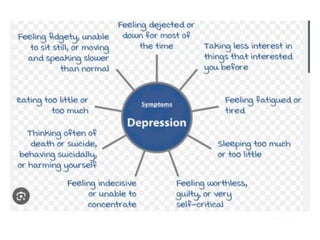
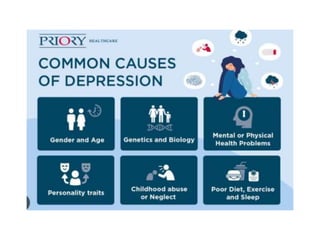
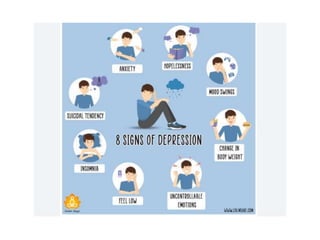
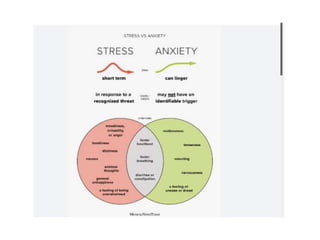
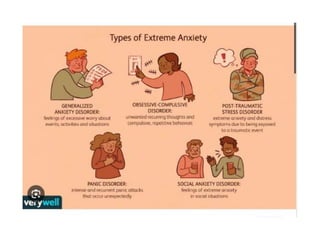
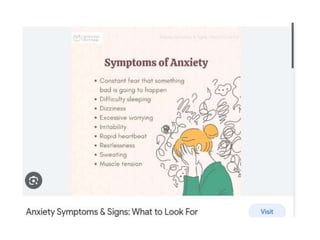
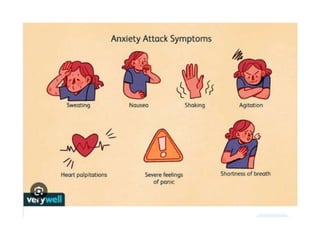
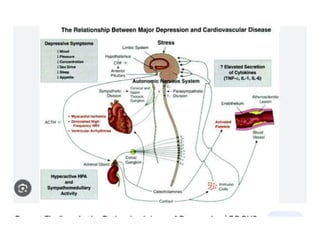
This document provides information on psychiatric disorders of depression and anxiety. It discusses the types, symptoms, causes, and treatments of different forms of depression like major depressive disorder, persistent depressive disorder, bipolar disorder, and seasonal affective disorder. It also covers anxiety disorders like generalized anxiety disorder, panic disorder, and social anxiety disorder. The document outlines biological, genetic, environmental, and hormonal factors that may contribute to the development of these conditions. Treatments discussed include psychotherapy, pharmacotherapy using antidepressants and anti-anxiety medications, and alternative therapies like exercise and supplements.

































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














