Downloaded 59 times
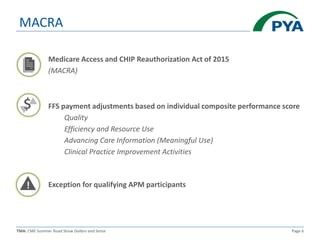
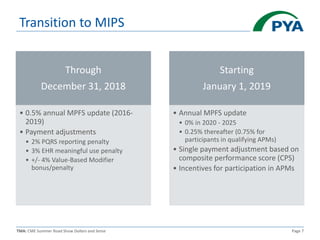
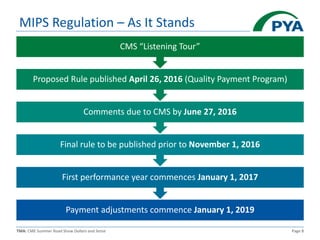
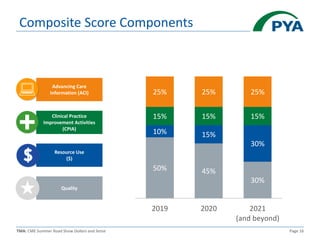
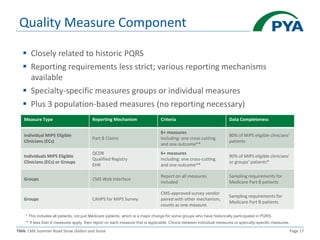
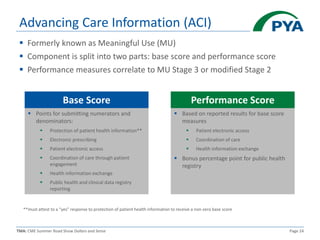
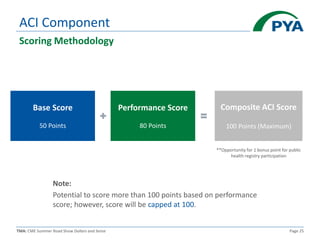
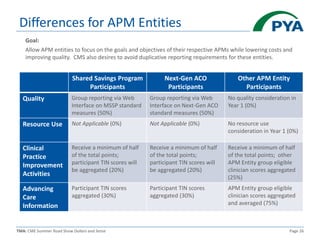
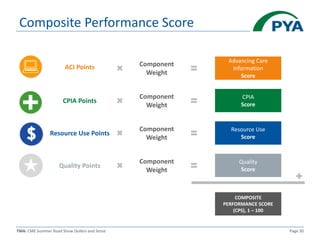
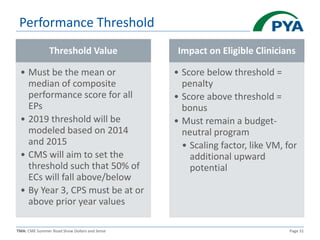
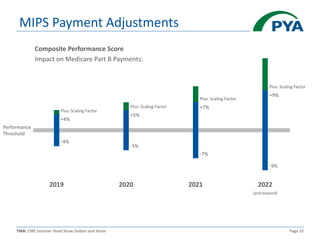
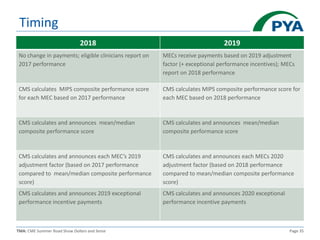


This document provides an overview of the Merit-based Incentive Payment System (MIPS) under the Medicare Access and CHIP Reauthorization Act (MACRA). MIPS replaces previous quality reporting programs and includes four components that determine a Composite Performance Score: Quality, Resource Use, Clinical Practice Improvement Activities, and Advancing Care Information. Scores will determine payment adjustments beginning in 2019, with the potential for bonuses or penalties up to 9% by 2022 based on performance compared to benchmarks and thresholds. The document reviews the scoring methodology and reporting requirements for each MIPS component.

















![Presentation on How to Encounter CMS & HHS RADV Audits [CEU]](https://cdn.slidesharecdn.com/ss_thumbnails/risk-adjustment-webinar-170810065012-thumbnail.jpg?width=640&height=640&fit=bounds)























































































