R Systems provides medical coding and risk adjustment services using a team of over 100 certified medical coders with at least 4 years of experience who are experts in CPT, ICD
# our igitalransformation artner
RISK A DJUSTMEN T CODIN G
2.
2
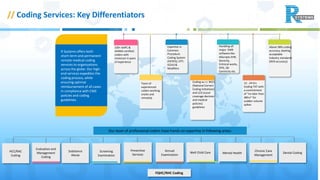
// Coding Services:Key Differentiators History
Our team of professional coders have hands-on expertise in following areas:
100+ AAPC &
AHIMA certified
coders with
minimum 4 years
of experience
Team of
experienced
coders working
onsite and
remotely
Coding w.r.t. NCCI
(National Correct
Coding Initiatives)
and LCD (Local
coverage decision
and medical
policies)
guidelines
12 - 24 hrs
Coding TAT with
a commitment
of “no later than
48hrs” for
sudden volume
spikes
Expertise in
Common
Procedure
Coding System
(HCPCS), CPT,
ICD10 &
Modifiers
Handling all
major EMR
software like
Allscripts EHR,
Sevocity,
Eclinical works,
EPIC, GE
Centricity etc.
Above 98% coding
accuracy, beating
acceptable
industry standards
(95% accuracy)
R Systems offers both
short-term and permanent
remote medical coding
services to organizations
across the globe. Our high-
end services expedites the
coding process, while
ensuring optimal
reimbursement of all cases
in compliance with CMS
policies and coding
guidelines.
Evaluation and
Management
Coding
Screening
Examination
Preventive
Services
Annual
Examination
Well Child Care Mental Health
Chronic Care
Management
FQHC/RHC Coding
Dental CodingSubstance
Abuse
HCC/RAC
Coding
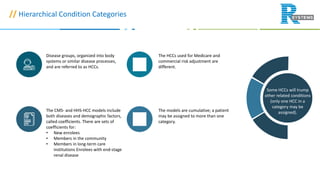
// Hierarchical ConditionCategories
Disease groups, organized into body
systems or similar disease processes,
and are referred to as HCCs.
The CMS- and HHS-HCC models include
both diseases and demographic factors,
called coefficients. There are sets of
coefficients for:
• New enrolees
• Members in the community
• Members in long-term care
institutions Enrolees with end-stage
renal disease
The HCCs used for Medicare and
commercial risk adjustment are
different.
The models are cumulative; a patient
may be assigned to more than one
category.
Some HCCs will trump
other related conditions
(only one HCC in a
category may be
assigned).
5.
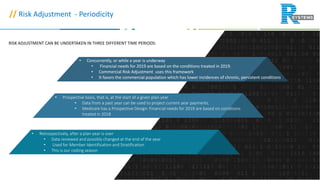
// Risk Adjustment- Periodicity
• Concurrently, or while a year is underway
• Financial needs for 2019 are based on the conditions treated in 2019.
• Commercial Risk Adjustment uses this framework
• It favors the commercial population which has lower incidences of chronic, persistent conditions
• Prospective basis, that is, at the start of a given plan year
• Data from a past year can be used to project current year payments.
• Medicare has a Prospective Design: Financial needs for 2019 are based on conditions
treated in 2018
• Retrospectively, after a plan year is over
• Data reviewed and possibly changed at the end of the year
• Used for Member Identification and Stratification
• This is our coding season
RISK ADJUSTMENT CAN BE UNDERTAKEN IN THREE DIFFERENT TIME PERIODS:
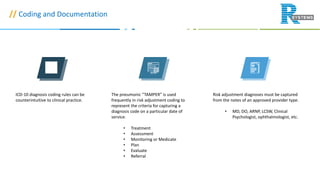
// Coding andDocumentation
ICD-10 diagnosis coding rules can be
counterintuitive to clinical practice.
The pneumonic “TAMPER” is used
frequently in risk adjustment coding to
represent the criteria for capturing a
diagnosis code on a particular date of
service.
• Treatment
• Assessment
• Monitoring or Medicate
• Plan
• Evaluate
• Referral
Risk adjustment diagnoses must be captured
from the notes of an approved provider type.
• MD, DO, ARNP, LCSW, Clinical
Psychologist, ophthalmologist, etc.
8.
// Coding andDocumentation
• Clinical documentation from inpatient hospital, outpatient hospital and face-to-face
office visits is acceptable for coding and reporting under risk adjustment.
• Examples of unacceptable documentation sources for risk adjustment coding/reporting
include:
• Super bills
• Referral forms
• Encounter forms
• Patient-only reported conditions
• Non face-to-face encounter notes
• Stand alone patient problem list
9.
// Common Error
Completeand accurate coding of the
most common conditions can have a
significant impact on risk capture
due to their prevalence . A few of the
prevalent conditions that are often
not monitored, evaluated, assessed
or treated and coded on an annual
basis are:
• Asthma
• Osteoporosis
• Hearing loss
• Psychiatric diagnosis: e.g. major
depression, bipolar disorder
• Vascular conditions: cardiac or
cerebral.
• These conditions can have a
significant impact on risk capture
due to their prevalence
Many high risk patients with multiple
conditions are often seen by a
specialist for the most severe or
symptomatic condition. However,
analysis shows significant coding
gaps for these relatively rare
conditions, which often require
specialty care, may be lost to care for
other conditions:
• Extremely or Very Low Birth
weight Neonates
• Respirator Dependence,
Tracheotomy status
• Haemophilia, Cystic Fibrosis
• Bone Marrow and Solid Organ
Transplant
• Severe Head Trauma
• Protein-Calorie Malnutrition














![Presentation on How to Encounter CMS & HHS RADV Audits [CEU]](https://cdn.slidesharecdn.com/ss_thumbnails/risk-adjustment-webinar-170810065012-thumbnail.jpg?width=640&height=640&fit=bounds)


























































