Downloaded 200 times



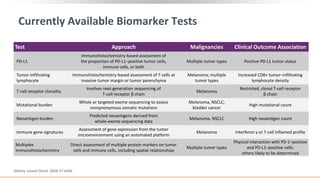
![BIOPSY: ESTABLISH DIAGNOSIS, DETERMINE
HISTOLOGIC SUBTYPE, BIOMARKER TESTING
• Histologic subtyping:
squamous or nonsquamous?[1]
• For biomarker testing:
• Primary tumors and metastatic lesions
equally suitable[2]
• Bone biopsy suboptimal due to
decalcification and degradation of DNA[2]
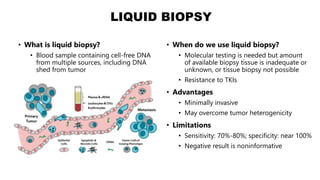
• Liquid biopsies (cell-free DNA in plasma) are
another option[3]
• Testing for PD-L1 expression
indicated in all NSCLC[4]
• Testing for EGFR, ALK, ROS1, BRAF
V600E, NTRK, RET, and METex14
indicated in all nonsquamous
NSCLC[4]
• Broad NGS testing encouraged to detect a
wider range of mutations using least amount
of tissue[4,5]
• For squamous NSCLC, consider testing in
young, never or light smokers, or if biopsy
specimen is small or of mixed histology[2]
• Completion of testing within 10-14 working
days of biopsy recommended[4,6]
• TAT for PD-L1 much shorter than for NGS
• Wait for results of NGS results
before acting on PD-L1 testing
results!](https://image.slidesharecdn.com/lungcancerppt-230813142821-85cb1605/85/lung-cancer-ppt-pptx-14-320.jpg)



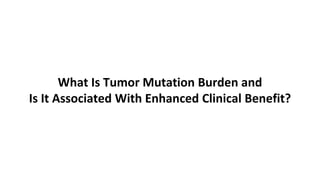
![High Tumor Mutation Burden May Influence
Immune-Mediated Antitumor Response
Tumor cells with
high TMB…[1,2]
…may have high
neoantigen load…[1,2]
…which can lead to
increased immune and
antitumor response[2-5]
1. Schumacher. Science. 2015;348:69. 2. Kim. Ann Oncol. 2016;27:1492. 3. Liontos. Ann Transl Med.
2016;4:264. 4. Sharma. Science. 2015;348:56. 5. Giannakis. Cell Rep. 2016;15:857.
The hypothesis that high TMB increases the
immunogenicity of tumors makes them a rational
target for treatment with I-O therapies[1,2]](https://image.slidesharecdn.com/lungcancerppt-230813142821-85cb1605/85/lung-cancer-ppt-pptx-35-320.jpg)


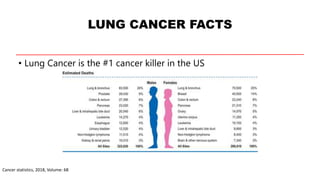
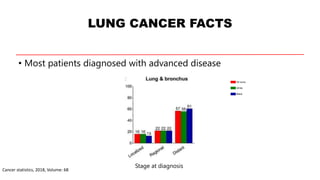
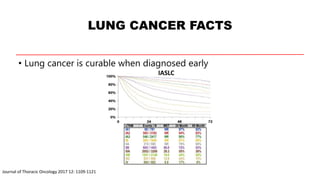
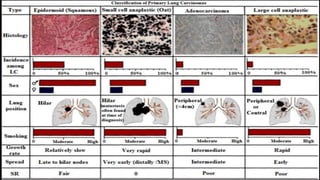
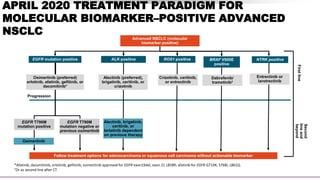
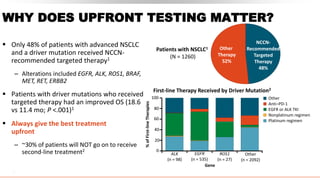
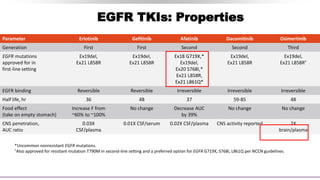
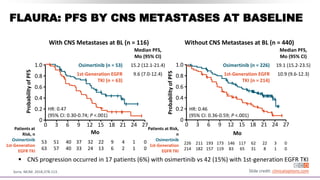
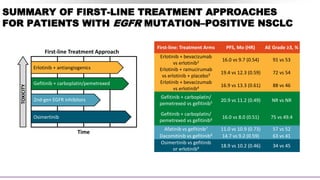
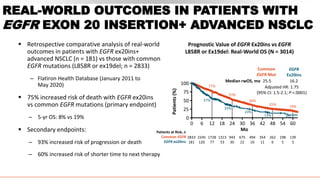
This document discusses recent updates in lung cancer. It begins by noting that lung cancer is the leading cause of cancer death in the US and is often diagnosed at an advanced stage. Screening with low-dose CT scans can detect lung cancer earlier and has been shown to decrease lung cancer mortality by 20% compared to chest x-rays. The National Lung Screening Trial established low-dose CT screening as an effective screening method for those at high risk. Biomarker testing is important to identify driver mutations and guide targeted therapy options, though barriers like tissue availability and turnaround time exist. Osimertinib has demonstrated superior progression-free survival compared to earlier EGFR TKIs for patients with EGFR-mut




































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)












![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)





