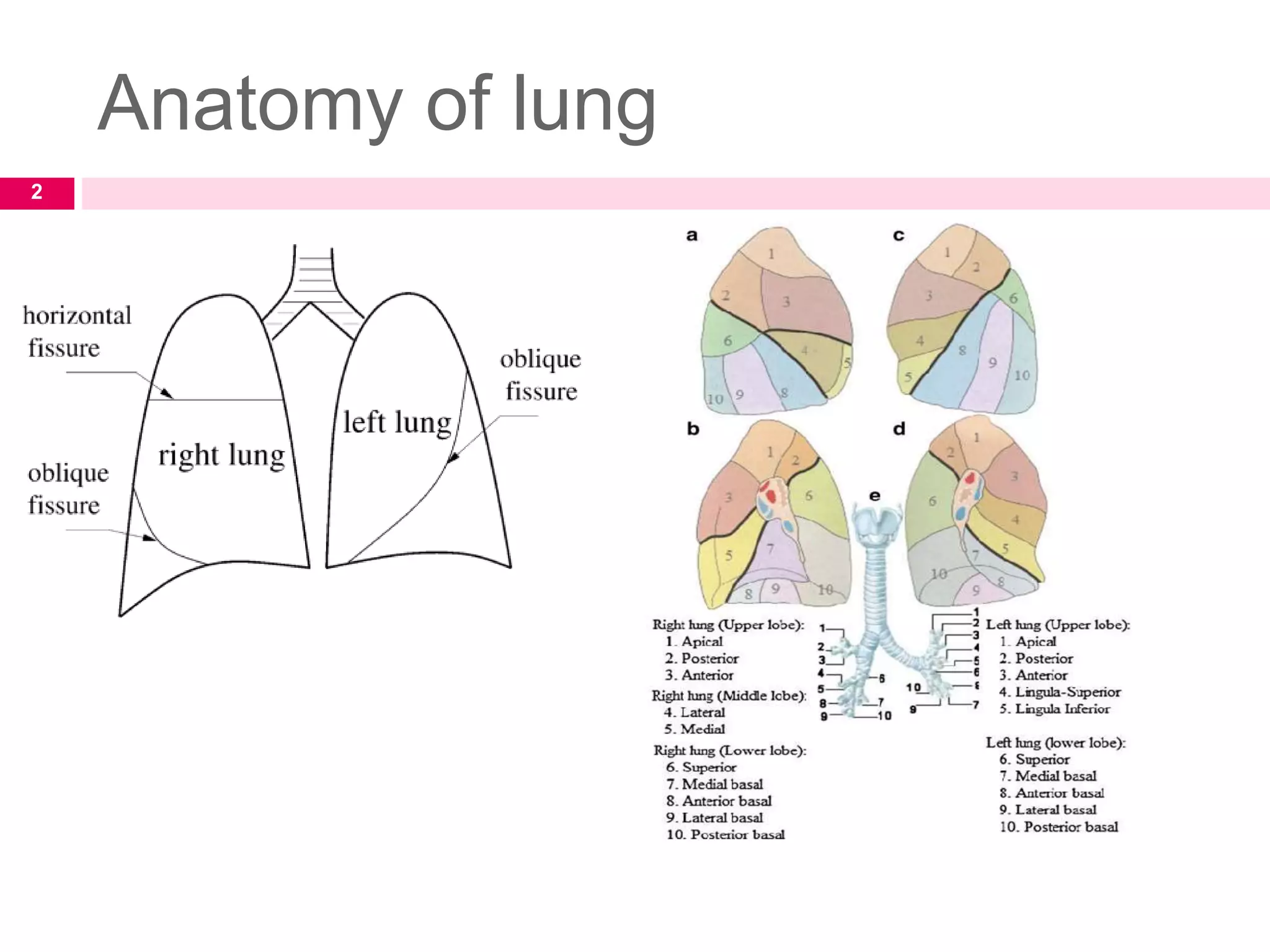
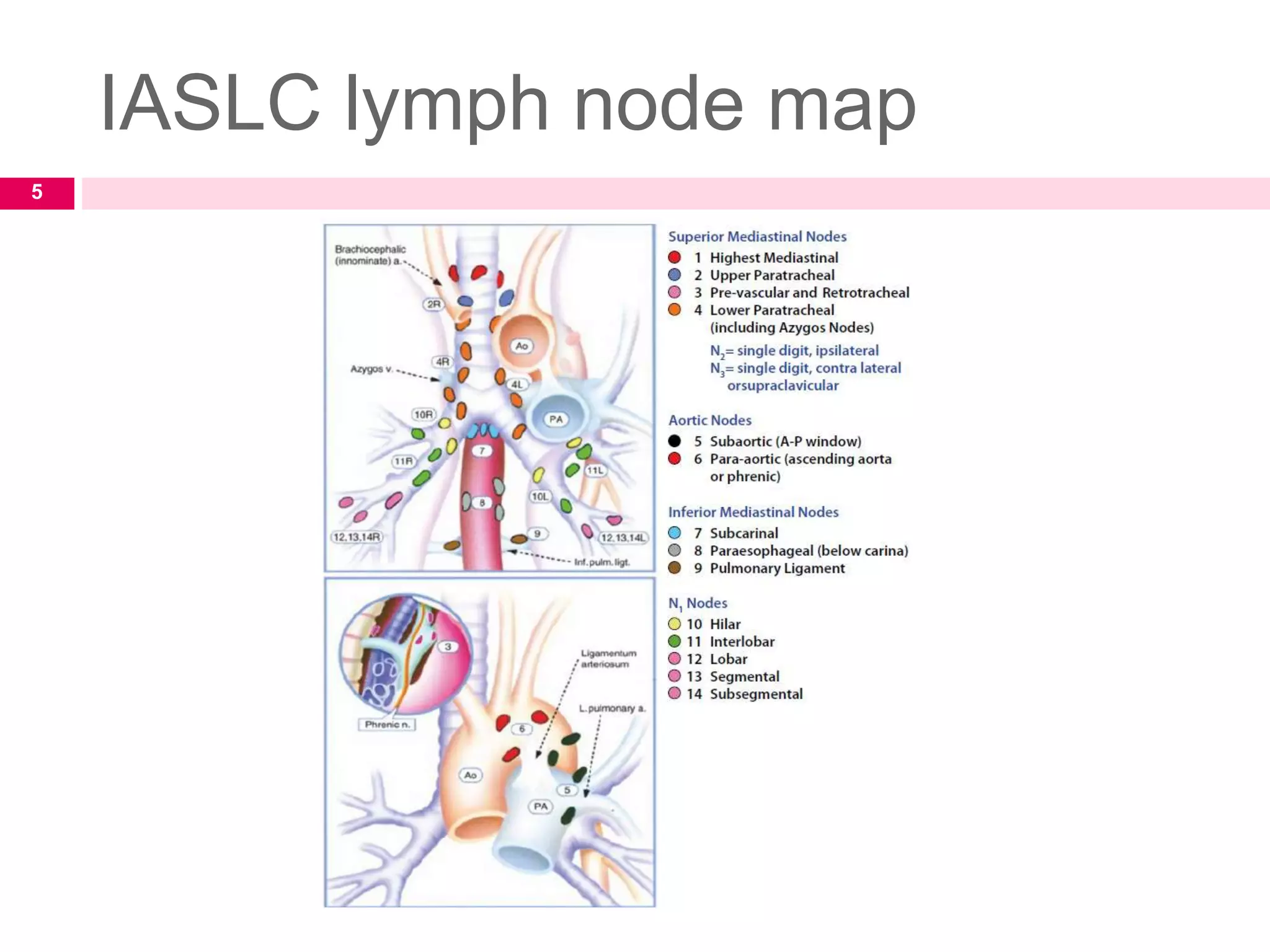
This document provides an overview of the management of non-small cell lung cancer (NSCLC). It discusses the anatomy of the lung and lymph node mapping. The clinical features, diagnostic workup including imaging and staging are covered. The various treatment approaches for early, locally advanced and metastatic NSCLC including surgery, radiation therapy, chemotherapy and targeted therapy are summarized. Techniques for radiation therapy planning and delivery such as 3D conformal radiation therapy, stereotactic body radiation therapy, proton beam therapy and brachytherapy are also outlined.