This document discusses lumbar pain and low back pain. Some key points:
- Low back pain is very common, expensive, and a leading cause of disability.
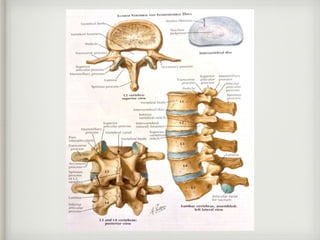
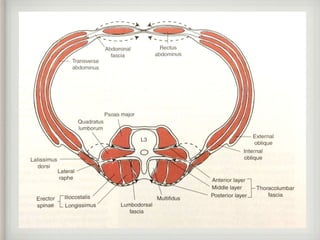
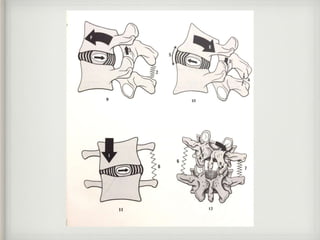
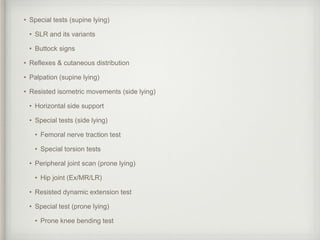
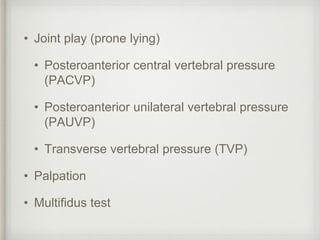
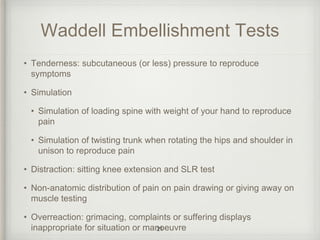
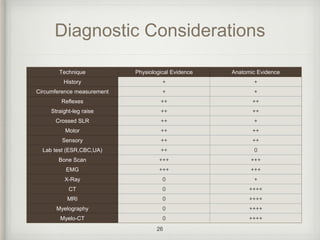
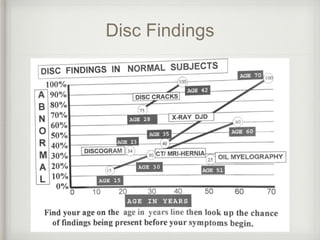
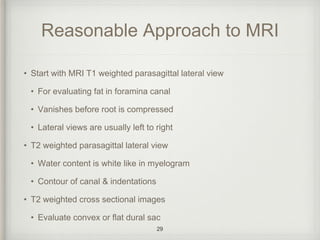
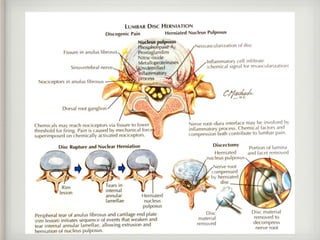
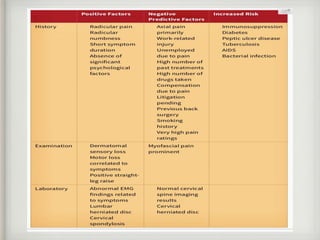
- Physical examination and imaging tests can help evaluate the source and severity of back pain.
- Treatments may include exercise, medication, injections, and in some cases surgery. However, surgery outcomes are often similar to non-surgical treatments.
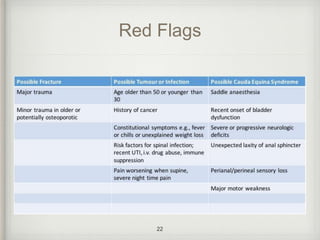
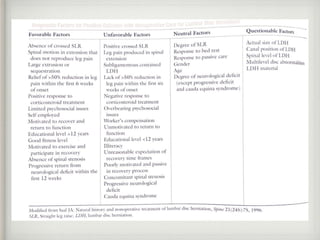
- Proper diagnosis is important to guide treatment, as many cases of back pain resolve on their own with time and conservative care.























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


