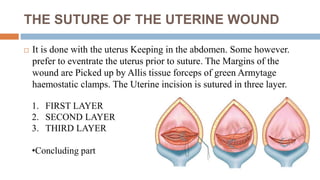
The document provides information about Caesarean section (C-section), including:
1. C-section is a surgical procedure to deliver babies through an incision in the mother's abdomen if vaginal delivery would put the baby or mother at risk.
2. The incidence of C-section is rising due to various factors like identification of at-risk fetuses/mothers, repeat C-sections, and decline in difficult vaginal deliveries.
3. Common indications for C-section include cephalo-pelvic disproportion, previous C-section, fetal distress, and breech presentation.
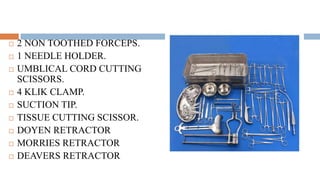
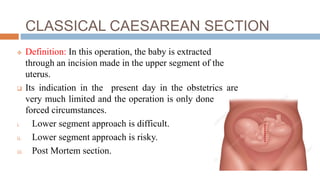
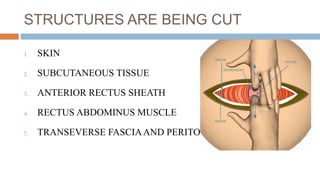
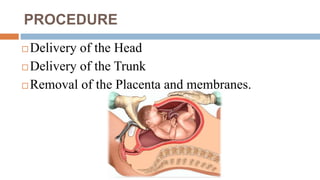
4. The procedure involves making an incision through skin, muscles and uterus to deliver the