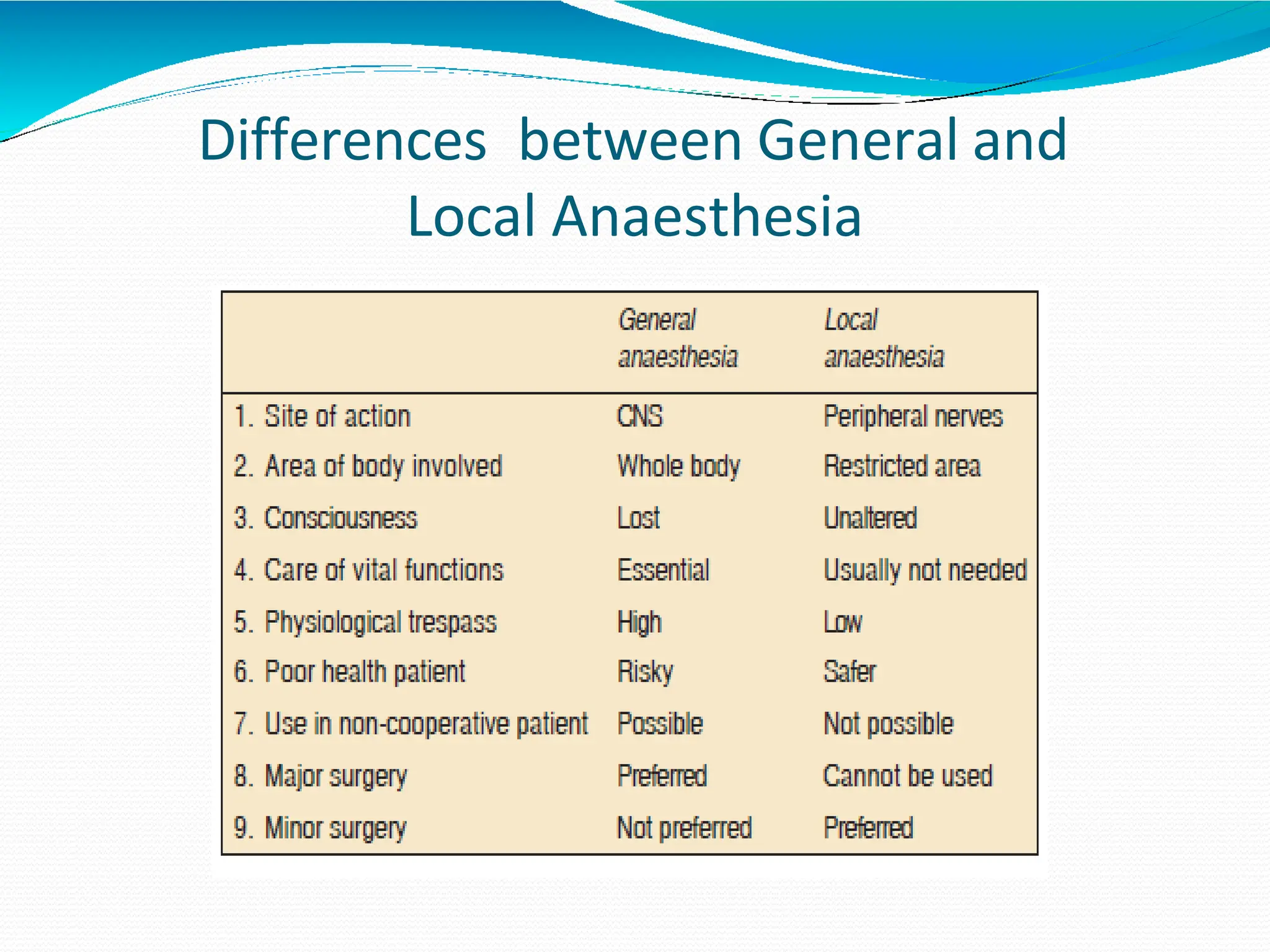
This document provides information on local anesthetics (LAs), including their classification, mechanism of action, effects, and uses. LAs work by blocking sodium channels in nerve cell membranes, preventing the generation and conduction of nerve impulses. They can produce local anesthesia through surface application or injection near sensory nerves or nerve trunks. Common LAs discussed are lidocaine, bupivacaine, and cocaine. Lidocaine is the most widely used due to its versatility, while bupivacaine provides longer-lasting anesthesia. Proper administration of LAs allows for anesthesia of specific body areas and structures.