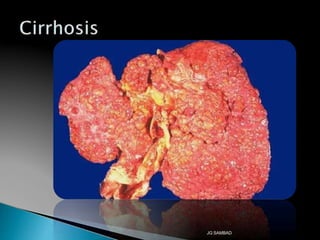
The document provides a detailed overview of cirrhosis, a chronic liver disease characterized by fibrosis, nodule formation, and progressive loss of liver function. It describes various causes of cirrhosis, including alcoholic liver disease, chronic hepatitis, and autoimmune conditions, along with the complications it can lead to, such as portal hypertension and hepatocellular carcinoma. Diagnosis typically involves liver biopsy and various laboratory tests, while imaging techniques like ultrasound are used to assess the condition of the liver.





























![Hepatic encephalopathy [HE]](https://cdn.slidesharecdn.com/ss_thumbnails/hepaticencephalopathy-200612174704-thumbnail.jpg?width=640&height=640&fit=bounds)








































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
