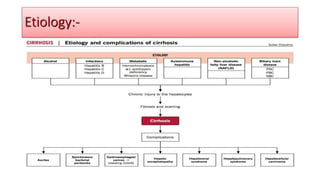
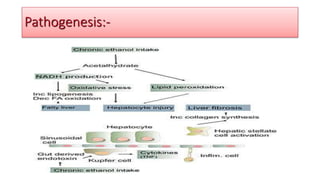
The document provides an overview of liver cirrhosis, including its definition, classification, signs and symptoms, etiology, complications, examination findings, diagnosis, differential diagnosis, and management. Cirrhosis involves scar tissue replacing healthy liver tissue and blocking blood flow through the organ. Chronic liver damage from hepatitis, alcohol abuse, and other causes can lead to cirrhosis. Patients may experience fatigue, weight loss, jaundice, bleeding, swelling, and confusion as the disease progresses. Management involves treating the underlying cause, medications, dietary changes, procedures like TIPS, and potentially transplantation.

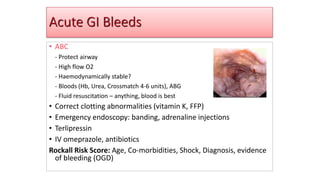
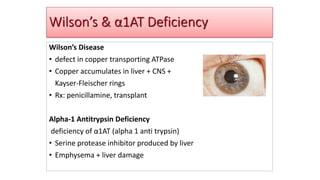
![Physical examination of patients with cirrhosis is usually remarkable for: jaundice, spider
angiomata, ascites, asterixis, spleenomegaly and palmar erythema.
• Appearance of the patient
• Patients with cirrhosis usually appear weak due to constitutional symptoms such as weight
loss, anorexia and muscle atrophy. Yellowish discoloration of skin and abdominal distension may
also be present due to ascites.
• Normal/low blood pressure with normal pulse pressure.
• Skin
• Jaundice : yellow discoloration of the skin, eyes, and mucus membranes due to
increased bilirubin (at least 2-3 mg/dL or 30 mmol/L). Urine may also appear dark.
• Pallor
• Bruises
• Palmar erythema on the thenar and hypothenar eminences, due to altered sex hormone
metabolism.
• Spider angiomata: Increased estradiol levels lead to the formation of vascular lesions consisting of
central arterioles surrounded by smaller vessels [1]
Examination:-](https://image.slidesharecdn.com/livercirrhosis-220925052246-e553225c/85/Liver-Cirrhosis-pptx-15-320.jpg)
![• Liver Biopsy
• Laboratory Findings
• Laboratory abnormalities may be the first indication of cirrhosis.
• Common abnormalities include:[1][2][3][4][5]
• Increased serum bilirubin levels[6]
• Abnormal aminotransferase levels [7][3][8][9][10][11][12][13][14][15][16]
• Elevated alkaline phosphatase
• Elevated gamma-glutamyl transpeptidase
• Prolonged prothrombin time/INR
• Thrombocytopenia
• Hyponatremia
• Liver function tests:
• Albumin:
• Albumin levels reflect synthetic function of the liver
• Serum albumin levels helps grade the severity of cirrhosis
• Hypoalbuminemia is non specific for liver disease and may be seen in:
• Bilirubin:
• Bilirubin levels may be normal or raised
• Prothrombin time: [27]
• Prothrombin time reflects the degree of hepatic synthetic function.
• Worsening coagulopathy correlates with the severity of hepatic dysfunction
Investigations:-](https://image.slidesharecdn.com/livercirrhosis-220925052246-e553225c/85/Liver-Cirrhosis-pptx-19-320.jpg)
![• .
• Metabolic panel:
• Hyponatremia[28]
• common in patients with cirrhosis and ascites and is related to an inability to excrete free water.
• Reflects poor prognosis
• Due to ADH elevation
• Progressive rise in serum creatinine: may be indicative of hepatorenal syndrome
• Hematologic abnormalities: [29]
• Thrombocytopenia: most common hematologic abnormality in cirrhosis
• Rarely results in a platelet count < 50,000/mL
• Mechanism of thrombocytopenia:
• caused by portal hypertension with congestive splenomegaly: sequesters circulating platelets
• decreased thrombopoietin levels
• Anemia](https://image.slidesharecdn.com/livercirrhosis-220925052246-e553225c/85/Liver-Cirrhosis-pptx-20-320.jpg)























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










