Downloaded 116 times








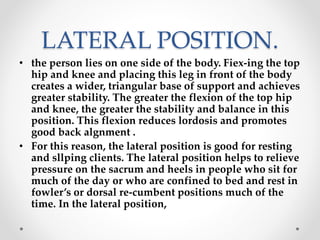
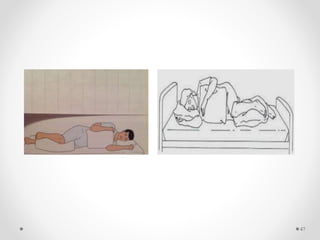


The document discusses proper techniques for lifting, moving, and positioning patients. It describes how to assess patients' needs and abilities before moving them, as well as correct body mechanics for nurses to employ, such as maintaining balance and a broad stance. Specific techniques are covered, including pulling, pushing, and pivoting patients. Different considerations are outlined for infants, children, and elders. Various patient positions like Fowler's position and lateral position are also defined. The goal is to safely move and position patients while preventing injuries to both patients and nurses.





























































































