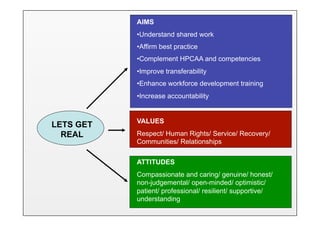
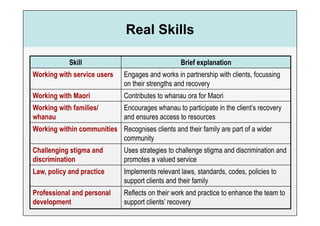
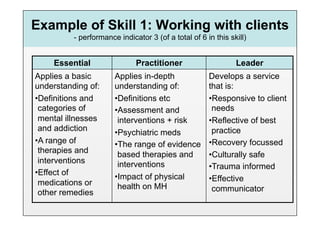
The document discusses the Lets Get Real framework for mental health and addiction treatment services. Lets Get Real describes seven skill sets, or "Real Skills", that practitioners should demonstrate at essential, practitioner, and leader levels. The goals of Lets Get Real are to improve services, ensure best practices, and increase accountability. It also aims to help different treatment services have a common language and perspectives on recovery-focused, culturally-capable care.






































































![Trauma Informed Care and Gambling [Part One]](https://cdn.slidesharecdn.com/ss_thumbnails/traumainformedcareandgamblingpartone-novideo-180327030806-thumbnail.jpg?width=640&height=640&fit=bounds)
































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



