Downloaded 83 times
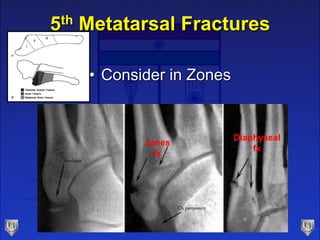
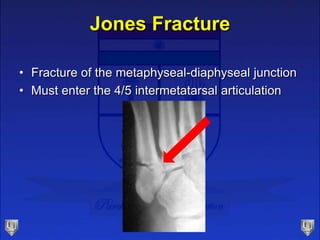


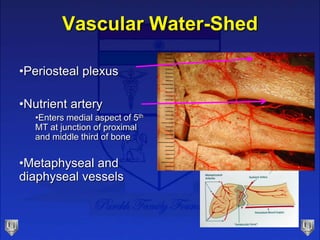


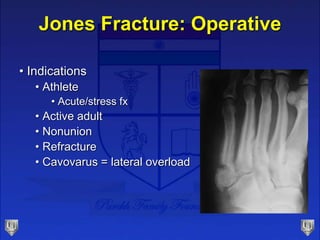
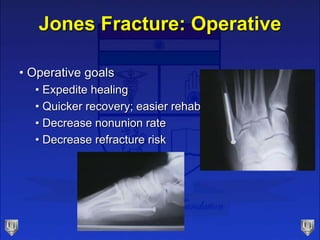
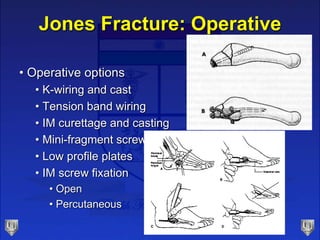
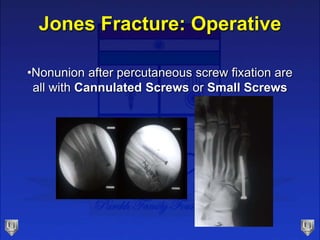

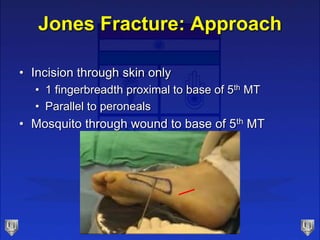
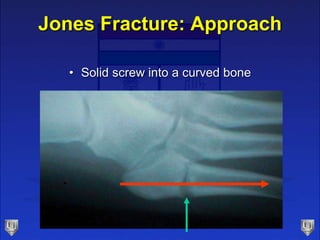
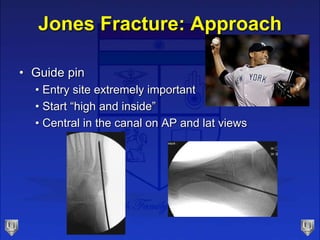
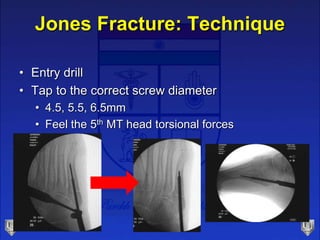


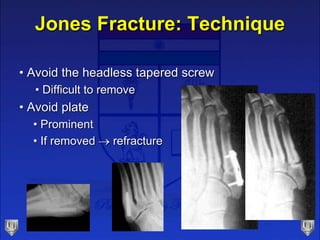
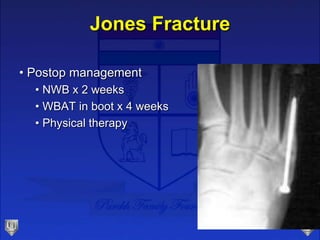
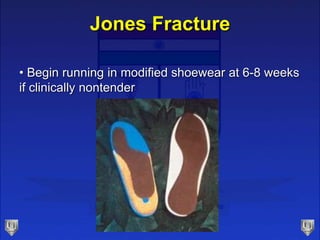
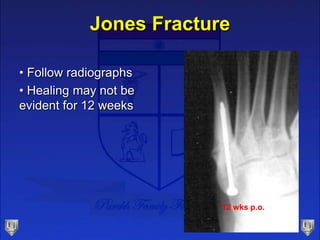
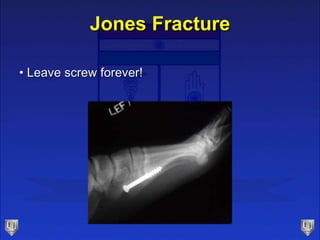
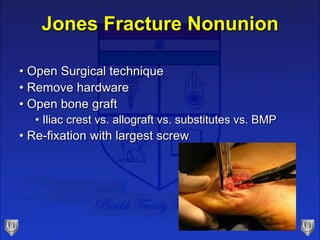
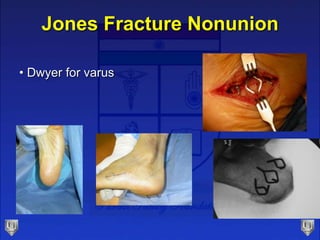

This document discusses Jones fractures, which are fractures of the metaphyseal-diaphyseal junction of the fifth metatarsal bone. It describes the anatomy and vascular supply of the region. Treatment options include non-operative management with casting for non-athletic patients or operative fixation with screws for athletes or active patients to expedite healing. The technique of percutaneous screw fixation is discussed, emphasizing the importance of starting the guidewire "high and inside" the bone. Postoperative management and potential complications are also reviewed.





















































































