
Recommended
Recommended
More Related Content
Similar to MANDIBULAR FRACTURES MANAGEMENT PROTOCO
Similar to MANDIBULAR FRACTURES MANAGEMENT PROTOCO (20)
More from EUROUNDISA
More from EUROUNDISA (11)
Recently uploaded
Recently uploaded (20)
MANDIBULAR FRACTURES MANAGEMENT PROTOCO
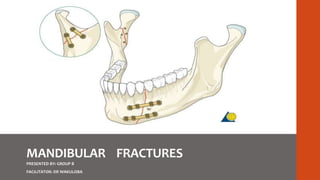
- 1. MANDIBULAR FRACTURES PRESENTED BY: GROUP B FACILITATOR: DR WAKULOBA
- 2. Contents. • Surgical anatomy • Epidemiology. • Classification systems • General Clinical features and diagnosis • Radiographic features • Management Principles
- 3. Surgical anatomy • Strongest facial bone • Parabola shaped bone • Angle of curvature is 110-140° • Mandible is the 2nd bone to ossify • Energy of 44.6-74.4 kg/m required to fracture the mandible.
- 5. Weak areas of mandible • Junction between alveolar bone & basal mandibular bone. • Symphysis region - junction of two individual bones. • Parasymphyseal region - lateral to the mental prominence, incisive fossa and mental foramen. • Junction of the ramus and the body are fractured commonly. • Presence of impacted tooth, canine with long roots.
- 6. Age changes of mandible. • Mental foramena. child – near inferior border. old age – near alveolar ridge. • Ramus angle. child & old – obtuse • Alveolar ridge • Blood supply
- 7. Champy’s principles • Forces of mastication produce tensional forces on upper border & forces of compression on lower border. • Champy put forward the lines where plates & screws have to be placed - “ideal osteosynthesis lines” • It corresponds to course of a line of tension at base of the alveolar process. • Only in symphysis region, 2 plates are placed to neutralize torsional forces.
- 8. Blood supply. • Helps in the healing of fractured bone. • Endosteal blood supply via inferior dental artery & veins. • Peripheral blood supply - Periosteum
- 9. Nerve supply. • Inferior alveolar nerve • Damage - angle & body # • Anesthesia or parasthesia of the nerve • Recovery / regeneration - 3 to 12 months
- 11. • Site
- 13. Classification • General • Anatomical • Completeness • Mechanism of injury • Number of fragments • Shape of fracture • Direction & favorability of treatment • Presence or absence of teeth • AO classification.
- 14. Kruger's Classification SIMPLE ( CLOSED) Linear fracture lines which do not communicate with the exterior COMPOUND ( OPEN) The fracture is communicating intraorally or extraorally. COMMUNITED Shattering of bone into multiple pieces
- 15. COMPLEX COMPLICATED There is adjunct injury to the adjacent nerves or major blood vessels , joints. IMPACTED One fragment is firmly driven within the other fragment and clinical movement not appreciated GREENSTICK Only one cortex broken. Common in children PATHOLOGICAL Spontaneous fracture as a result of normal muscle contraction or trauma due to increased weakness of underlying bone . Impacted fracture
- 16. Dingman and Natvigs Classification • Symphysis fracture • Canine region fracture • Body of the mandible fracture • Angle fracture • Ramus fracture • Coronoid fracture • Condylar fracture • Dentoalveolar fracture
- 17. Direction & favorability of treatment Horizontally Favourable Fracture line runs downward & forward so upward displacement avoided Horizontally Unfavourable Fracture line runs Down Wards and Back Wards so upward Displacement Unrestricted
- 18. VERTICALLY FAVORABLE VERTICALLY UNFAVORABLE FRACTURE LINE RUNS FROM THE OUTER BUCCAL PLATE OBLIQUELY BACKWARDS AND LINGUALLY , MEDIAL MOVEMENT RESTRICTED FRACTURE LINE RUNS FROM THE INNER LINGUAL PLATE OBLIQUELY BACKWARDS AND BUCCALLY , MEDIAL MOVEMENT UNRESTRICTED
- 19. Presence or absence of teeth Kazanjian V.H. & Converse J.M. CLASS 1 TEETH ON BOTH SIDES OF FRACTURE LINE MONOMAXILLARY CLASS II TEETH ONLY ON ONE SIDE OF THE FRACTURE LINE INTERMAXILLARY FIXATION CLASS III EDENTULOUS PATIENT OPEN REDUCTION / PROSTHESIS
- 20. AO Classification F NO. OF FRACTURE OR FRAGMENTS L LOCATION OF THE FRACTURE O STATUS OF OCCLUSION S SOFT TISSUE INVOLVEMENT A ASSOCIATED FRACTURES
- 21. F: NO. OF FRACTURES F0 Incomplete fractures F1 Single fractures F2 Multiple fractures F3 Comminuted fractures F4 Fracture with bone defect
- 22. L: Location of fracture L1 Pre-canine L2 Canine L3 Post-canine L4 Angle L5 Supra-angular L6 Condyle L7 Coronoid L8 Alveolar process
- 23. O: Status of occlusion O 0 No malocclusion O 1 Malocclusion O 2 Edentulous mandible
- 24. A: Associated fracture A 0 None A 1 Dentoalveolar fracture A 2 Nasal bone fracture A 3 Zygoma fracture A 4 Lefort I A 5 Lefort II A 6 Lefort III
- 25. Clinical examination. • History • Mechanism of injury • Extraoral / Intraoral
- 26. Clinical features. • Extensive edema • Tenderness. • step deformity • bone crepitus • Facial asymmetry
- 27. Deviation of jaw Restriction of mouth opening
- 28. Extensive soft tissue and bony defect
- 29. Collapsed arch and Interfragmentary mobility Open bite due bilateral poster Gagging of occlusion Open bite and cross bite due to Unilateral gagging of occlusion Occlusal step with Unilateral cross bite
- 30. Mandibular fracture has to be differentiated from extensive Soft tissue injury and dentoalveolar trauma UNILATERAL CROSS BITE UNILATERAL OPEN BITE
- 31. Multiple fragmentation With complete loss of occlusion Sublingual hematoma Unfavorable fracture line Causing displacement
- 32. Displacement of fracture • Direction and intensity of the traumatic force. • Site of fracture. • Direction of fracture line. • Muscle pull exerted on fractured fragments. • Presence or absence of teeth. • Extent of soft tissue wound.
- 33. Radiographic Investigations OPG PA View PNS View(Paranasal sinuses ) Lateral oblique Radiograph Occlusal view CT scan.
- 34. - Commonly used. - Entire mandible is visualized. OPG view
- 35. PA view. • Medial / lateral displacement.
- 36. lateral view, occipital frontal (OF) view and finally the occipital mental (OM) view Indicated for Visualizing Medial Displacement Of Condylar Neck The 4th & 5th MacGregor Line coincides with Mandible PNS view
- 37. Because of distortion in Symphysis Region in an OPG , an Occlusal View is indicated in Symphysial fractures Also shows Vertical Favorability of Body Fractures Occlusal view
- 38. CT scan. • Condylar fracture. • Cervical spine injury.
- 39. Principles of Management of mandibular fractures
- 40. Principles of management • Aim of intervention- restore the fracture segments to their pre-fracture position and rigidly hold the segments together long enough for them to unite. This is known as reduction and fixation. • The principle of management- adequate reduction and fixation of the reduced segments to allow for primary healing or formation and stabilization of the bone callus at the fracture site followed by rehabilitation. • Basic principles: Reduction Fixation Immobilization
- 41. Definition • Reduction refers to the repositioning of the fractured bony segments into the preinjury normal anatomical position. • The reduction can be achieved by withot exposure of the fracture site; closed reduction(CR) or by direct exposure and approximation of the fractured segments; open reduction(OR). • The reduced fracture segments can be fixed internally by either; Rigid fixation Semi-rigid fixation • Or fixed externally by either; Extraoral methods as in frames Intraoral as in MMF or splints
- 42. 1.Conservative management. Criteria: 1. Where there is a linear un-displaced fracture. 2. Occlusion not affected by the fracture. 3. No infection evident in the fracture site. 4. Compliant pt willing to be on prescribed soft diet for atleast 4 weeks. 5. Coronoid fractures that do not cause restriction of mouth opening or closure. • Pain management and prophylactic antibiotics • Instructions on how to maintain good OH.
- 43. Closed reduction • Refers to external fixation devices and maxillomandibular fixation(MMF), also referred to as intermaxillary fixation(IMF). • Based on the principle that when the teeth on fractured segments are in correct occlusion with the opposing maxillary teeth, then the bone fragments to which they are attached will also be satisfactorily aligned. • Healing of the bone occurs by secondary intention with callus formation and takes 4-6 weeks • The presence of teeth provides an accurate guide for reduction. • Teeth may on occasion be brought into contact during reduction, yet be occluding incorrectly owing to lingual inclination of the fractured fragments. • Whenever the occlusion is used as an index of accurate reduction, it is important to recognize any pre-existing occlusal abnormalities, such as anterior open bite, etc. • Wear facets on the teeth, can provide valuable clues to previous contact areas
- 44. Indications for CR of a mandibular fracture 1. Non-displaced favorable fracture. 2. Grossly comminuted fractures with small bone fragments where stripping of the periosteum from the small fragments may lead to necrosis. 3. Severely atrophic edentulous mandible. 4. Lack of soft tissue overlying the fracture site. 5. Fractures in children with developing teeth buds. 6. Coronoid process fractures 7. Pts deemed as high risk for treatment under GA. 8. Pts who cannot afford ORIF. Contraindications of CR • Pts with poorly controlled seizure history like epilepsy • Compromised pulmonary function( moderate to severe asthma, COPD) • GIT disorders(GERDS)
- 45. Techniques and materials used to achieve MMF: Archbars Interdental wires(eyelets or ivy loops) Reduction by use of elastic traction; Severely displaced fractures maybe difficult to reduce into occlusion, hence rubber elastics may be used between the hooks on the lower and upper arch bars instead of tie wires. These are used for 3-7 days as a temporary measure to gradually guide the fractured segments into occlusion.
- 49. Disadvantages of MMF • Requires an extended period of immobilization • May pose a problem to the airway. • Poor nutrition and weight loss • Poor OH • Phonation and speech difficulties • May lead to difficulty in recovering normal range of jaw mvmt. • Ankylosis in children • Requires the presence of a sound dentition • Social inconvenience and discomfort. • Subsequent muscle disuse atrophy.
- 50. Open reduction and internal fixation(ORIF) • Open techniques involves surgical exposure of the fracture site and direct fixation at the fracture site once reduction is achieved. • Fracture segments are brought too their correct position before fixation which can be attained by MMF in pts with adequate dentition or by manipulation using reduction forceps in edentulous or compromised dentition status. • Can be intraoral or extraoral depending on the location and severity or complexity of the fracture. • Extraoral approach, through a submandibular incision(>4 cm below the inferior margin of the mandible to minimize the risk of the marginal mandibular nerve injury).
- 51. • ORIF can be achieved by either semi-rigid fixation or rigid fixation. 1. SEMI-RIGID FIXATION Also, direct wire osteosynthesis(DWO) A form of fixation using 0.35mm-0.6mm SS wire to secure the fractured segments. A small amount of movement of the proximal and distal segments occurs causing healing with periosteal callus formation. Requires superior and inferior border wiring and must remain reinforced with MMF for atleast 4 weeks. Useful in angle and parasymphyseal fractures in centers where reconstruction plates are not available or affordable. 2.Rigid fixation Involves the use of plates of varying sizes and shapes that are selected based on the fracture site and severity. Once acceptable reduction is achieved, the selected plate is bent appropriately and adapted to the bone. The plates are then secured in place using screws that are measured to match the thickness of the mandible at that point.
- 52. Methods of fixation after open reduction 1. Direct wire osteosynthesis 2. Circum-mandibular wire. 3. Mini-plates and monocortical screws 4. Rigid plates and bi-cortical screws 5. Rigid compression plates and screws 6. Lag screws(in parasymphyseal region)
- 53. (1)Preoperative X-ray showing fracture line, (2)Extraoral open reduction, (3)Compression bone plate adaptation and fixation after reduction, (4) Compression bone plate fixed with bicortical screws, (5) Postoperative X-ray showing rigid fixation
- 54. Indications for open reduction 1. Displaced unfavourable fractures through the angle of the mandible 2. Pts with concurrent displaced mid-face fractures(panfacial) where a rigid mandible is necessary 3. Fractures of a severely atrophic mandible that requires primary bone grafting. 4. Multiple fractures. 5. Malunion 6. Non-union 7. Pathologic fractures 8. Some condylar fractures 9. Pts with conditions in which CR is contraindicated.
- 55. Contraindications for open reduction 1. Pts who are high GA risks. 2. Atrophic edentulous mandible where periosteal stripping may lead to necrosis. 3. Comminuted fractures with tiny bone fragments. 4. Children at risk of damage to the unerupted permanent dentition. 5. Some condylar fractures 6. Inadequate facility and lack of a skilled surgeon
- 56. Absolute and relative indications of OR by Zide and Kent Absolute indications • To restore vertical and anteroposterior facial dimension. • When stability of occlusion is limited • When rigid internal fixation is used to address other facial fractures affecting the occlusion • When manipulation and closed treatment cannot re-establish the pre-traumatic occlusion. • Invasion of foreign body. • Post pubertal pts • Dislocation of the condyle into middle cranial fossa. Relative indications • Edentulous jaws • Uncontrolled seizure disorders • Status asthmaticus • Psychologic compromise
- 57. Advantages of ORIF 1. Immediate loading of the mandible is possible within 1-2 weeks. 2. No prolonged period of immobilization. 3. Good OH practice possible. 4. Pt is able to take normal oral medication. 5. Speech is not interfered with. 6. Where CR has failed.
- 58. Disadvantages of ORIF 1. GA related risks. 2. Expensive(reconstruction plate and theatre) 3. Implant may cause foreign body reaction. 4. 2nd operation to remove the implant may be necessary. 5. Risk of damage to nerves. 6. scarring(keloids and hypertrophic scars) 7. Not compatible with MRI if steel based 8. Damage to deciduous dentition in children. 9. Risky in pts with bleeding disorders 10. Atrophic edentulous mandible may undergo necrosis due to peristeal stripping.
- 60. Coronoid fracture • Rare fracture-Isolated fractures of the coronoid process caused by direct trauma are rare, as it is anatomically protected by the complex zygomatic arch/ temporo-zygomatic bone and their associated muscles. (2.9% of the mandibular fractures) Aetiology • Most fractures here are caused by strokes (contusion or penetrating injuries) • Caused by reflex contraction of temporalis or direct trauma to ramus. • Fragment pulled upward into the infratemporal fossa
- 61. Clinical features • Tenderness over the anterior ramus • Painful limitations of extrusive and lateral excursive movement. • Slight to moderate swelling over the region of the zygomatic arch. • Malocclusion • Conservative management is first recommended for fractures of the coronoid process with minimal displacement or restriction of mouth opening. • For patients with significant fracture displacement and limited mouth opening, or with concomitant fractures of the zygoma, zygomatic arch, or mandibular ramus, ORIF via the modified retromandibular approach through the anterior border of the parotid gland is an alternative treatment method.
- 63. Angle fractures • The angle of the mandible is an anatomically weak and an area susceptible to fracture. The presence of an impacted or partially erupted third molar tooth further weakens it. • Angle of mandible is the most common site for fracture (23-42% of mandibular fractures) however, bilateral angle fracture is very rare and uncommon. • Causes-motor vehicle accident, assault • Classification depends on the direction of the fracture line and the effect of muscle action • Hence fractures are • Vertically favourable or unfavourable • Horizontally favourable or unfavourable
- 65. • Muscles attached to the ramus –the masseter, temporalis and medial pterygoid displace proximal segment upward and medially when the fractures are unfavourable. • The muscles also impact the bone minimizing displacement in horizontal and vertical favourable fractures
- 66. Inspection • Swelling at the angle with obvious deformity • Step deformity behind the last molar • Haematoma adjacent to the angle on either the buccal and lingual side • Anaesthesia or paresthesia of lower lip • Derangement of occlusion.(anterior open bite, retro gnathic occlusion) Palpation • Tenderness at the angle externally • Movements/crepitus at the site • Step deformity • Painful movement /trismus • Loose teeth
- 67. Management 1.Closed reduction and intermaxillary fixation for 4-6 weeks with arch bars,screws.Indicated in simple fractures without any significant displacement 2.Open reduction Indicated in unfavourable fractures with significant displacement. Two fracture lines at the base Periodontally compromised teeth Edentulous patients Open reduction and non-rigid fixation with wire Open reduction and rigid external fixation with plates and lag screws.
- 68. Open reduction with upper border wiring and MMF Advantages • Minimally invasive • Requires less skill • Economic Disadvantages • Non rigid • Has to be removed • Possibility of lingual nerve injury
- 69. Open reduction with rigid fixation • Rigid fixation is associated with rapid bone healing,excellent stabilization at fracture site and excellent post –operative stability. Disadvantages of rigid fixation • Bicortical screws used cause sensory disturbance along the path of the inferior alveolar nerve • Post-operative malocclusion rates are high due to difficulties in bending the rigid plate. • Extra oral scar due to incisions made in the extra oral approach.
- 72. • Upper border plate/tension plate on the external oblique ridge • Indicated for vertical and horizontal favourable fractures Upper and lower plate • Considered the best line of treatment • Used in all types of fractures. • Plate size and rigidity depend on the direction of the force
- 73. • Open reduction with 3 dimension plates • Acts as double plating • Prevents torsion movement • Plate placed at the mandibular angle 2.0mm titanium plate
- 74. • Reconstruction plate with other methods of fixation. • Best used in comminuted fracture
- 75. Surgical approaches • Intraoral approach incision on external oblique ridge • Submandibular incision • Incision through the laceration
- 76. Body fracture-Molar and premolar region Aetiology- fracture of the body of the mandible accounts for almost 11% to 36%, with personal violence as the principal factor. Epidemiology • In children, condylar and body fractures have been demonstrated to be the most prevalent maxillofacial fractures. • Body fractures are more prevalent among males than females. • Mandibular body fractures usually occur between the distal aspect of the canine and a hypothetical line that corresponds to the region of anterior attachment of the masseter muscle. • They may be classified based on the anatomic location, the direction of the fracture line, position of teeth relative to the fracture, and favourability. • Based on the fracture line direction and the effect of muscle distraction on the fracture fragments, the body fractures can classify into two types (favorable and unfavorable).
- 77. • In favorable fractures, the bony fragments are drawn together by the muscle distraction, whereas in unfavorable fractures, the bony segments become displaced by the muscle forces. • These forces that render the fracture unfavorable are exerted by various muscles such as masseter, temporalis, and medial pterygoid muscle. These muscles distract the proximal bony segment in the superomedial direction. • Moreover, two additional muscles (mylohyoid and anterior belly of digastrics) may also play a role in displacing the segments in the posterior and inferior direction.
- 79. Physical examination • Intraorally, a change in occlusion may be apparent on physical examination. • There may be anaesthesia, paraesthesia, or dysesthesia of the lower lip. This change in lower lip sensation generally occurs in displaced body fractures that are distal to the mandibular foramen (along with the distribution of the inferior alveolar nerve) and not seen in nondisplaced mandible fractures. • Laceration in the gingiva, • Step defect in the occlusion, • Ecchymosis in the mouth floor is a pathognomonic sign of a mandibular body fracture. • The examiner should note the mobility in the fracture. To do so, use both hands to manipulate the mandible by placing the thumb on the occlusal surface of the teeth and fingers on the inferior border of the mandible. Then slowly and carefully, pressure should be placed between the two hands.
- 80. • Extraorally, there may be a change in facial contour due to loss of external mandibular form and skin abrasion. • flattened appearance of the lateral aspect of the face. On palpation of there is a loss of the mandibular body. An unfavorable fracture should be suspected. • The anterior face may get displaced in the forward direction, resulting in elongation. In such cases, the anterior mandible becomes displaced in the downward direction.
- 81. Evaluation • Evaluation of the body fracture is via radiographs using plain radiography (panoramic, lateral-oblique, posteroanterior, occlusal, and peri apical views) and CT scan. • The lateral-oblique view helps to diagnose posterior body fractures. • Mandibular occlusal view and Caldwell posteroanterior view demonstrate the presence of medial or lateral displacement of body fractures. • Among all the radiographs, the most informative is the panoramic radiograph. • CBCT can be useful as it is highly sensitive in identifying fractures. Also, it provides better imaging quality and decreases the chances of interpretation error
- 82. • There are two methods to treat mandibular body fractures, i.e., non- surgical conservative management and surgical management. Whether to treat the fracture using surgical or non-surgical means depends on the type, severity, and consequences of fracture. Indications for closed reduction include: • Non-displaced favorable fractures • Presence of healthy dentition with sufficient teeth to obtain a stable occlusion • Grossly comminuted fractures • Edentulous fractures • Fractures in children with developing dentition • Presence of adequate occlusion • Good facial esthetics and adequate open mouth
- 83. Open reduction and internal rigid fixation (ORIF) • Surgical management can take place using an intraoral or extraoral approach, the choice of which depends mainly on the site and type of body fracture. • Simple and fractures in the anterior segment with no or only slight dislocation should preferably have treatment using an intraoral approach. This approach provides excellent access to the fracture site and allows observing the occlusion to reduce fracture and application of rigid fixation. • The incision is placed in the vestibular region approximately 5 to 7 mm below the mucogingival junction to facilitate closure. This location also aids in the prevention of wound dehiscence. During an intraoral approach, care is necessary to avoid injuring the mental nerve. On the other hand, the clinician can treat comminuted and fractures in the posterior segment with a high degree of dislocation using an extraoral approach as placing longer and stronger plates is difficult using the intraoral approach. An extraoral surgical approach is also a possibility with fractures that lie between the mandibular body's inferior and lingual aspects. Care is necessary to avoid injuring the marginal mandibular nerve
- 84. Prognosis • Both closed and open reductions of mandibular body fractures lead to favorable results in terms of bony union. • The treatment of dental injuries should be done concurrently with the fracture as the fractured teeth may become infected and jeopardize bone union. • Hence, they require removal. • As mandibular canines help to determine the occlusion, the clinician should preserve them, if possible. • The management and prognosis of edentulous body fractures are often challenging due to advanced age and multiple comorbidities.
- 85. Symphysis and parasymphysis fractures • Symphyseal/parasymphyseal fracture is defined as fracture line in mandibular bone between the canine teeth. • The symphysis of the mandible is defined as the region between the roots of the central incisors, and the parasym- physis as the region between the lateral roots of the canines and the central incisors. • Mandibular symphyseal fracture accounts for 15.6 to 29.3% of mandibular fractures • Commonly associated with fractures of one or both condyles. • Aetiology Trauma from interpersonal violence or motor vehicle accidents. Falls, industrial accidents, and sports injuries are lesser etiologies. Most trauma is blunt, but penetrating trauma is common with interpersonal violence and war injury.
- 86. Pathophysiology • Blunt trauma can injure any part of the mandible. • A sharp blow applied anteriorly often fractures the symphyseal/parasymphyseal region and the condyle region or regions. • Blunt force applied broadly across the body of the mandible may also result in a fracture of the symphyseal/parasymphyseal region.
- 87. Clinical features of symphyseal and parasymphyseal fractures • Tenderness at fracture site. • Lingual haematoma(Cole’s sign) • Inability to control salivary secretion. • In oblique fractures,there is overriding of the segments with lingual inversion of the occlusion. • Soft tissue injury of the lip and chin. • Detachment of the genioglossus muscle-Loss of tongue support and obstruction of the airway. • Not usually associated with anaesthesia of the Mental region • Possible condylar fracture
- 88. Management of symphyseal and parasymphyseal fractures • Closed reduction • Open reduction with inernal fixation using cortical plates in displaced fractures
- 89. Fractures of the edentulous mandible • Fractures of the edentulous mandible pose unique challenges. The atrophic mandible has little osteogenic potential and a reduced healing capacity . • In the past, MMF was used by wiring the edentulous mandible to dentures or splints. However, because these patients are often elderly with comorbidities, it created additional complications such as infection and pulmonary issues • Rigid, internal fixation is frequently performed in these patients . This has led to reduced convalescence time and a more manageable healing process. • Primary bone grafting is commonly done because of the atrophic nature of the mandible.
- 90. • Options for ORIF include the use of miniplates or larger locking reconstruction types . • Miniplates are small in size, which allows for smaller incision sites. • The screws are also small, which allows these plates to be placed in areas of thin bone fragments, such as in the edentulous mandible. • Both single and double miniplates can help with load sharing in mandibular fractures. • For larger fractures, heavier, load-bearing locking plates can be used. This helps with flexion in the mandible that occurs with opening and closing the mouth, which especially affects the edentulous mandible.
- 93. Mandibular fractures in children • Mandibular fractures in children most commonly occur in condylar region, followed by para-symphysis and angle. • The fractures tend to be minimally displaced and in majority of cases can be treated conservatively. • Young bone possesses unique physical properties that coupled with space occupying developing dentition give rise to patterns of fracture not seen in adults. • Bone fragments in children may become partially united as early as 4 days and fractures become difficult to reduce by seventh day.5 • This results in need for different forms of fixation as early as possible for comparatively shorter duration of time.
- 94. • Non-union or fibrous union rarely occurs in children and excellent remodelling occurs under the influence of masticatory stresses even when there is imperfect apposition of bone surfaces. • The management of mandibular fractures in children differs somewhat from that of adults mainly because of concern for possible disruption of growth • Growth abnormalities may occur as result of fracture dislocation of condyle due to elimination of ‘functional matrix’ of lateral pterygoid function, trismus or ankylosis. • Methods of dentoalveolar stabilization also require some reforms. Between 2-4 years sufficient number of fully formed deciduous teeth are present facilitating application of arch bars or eyelet wires. • 5 to 8 years age old group may present with some difficulty owing to loss or loosening of deciduous teeth. • The shape and shortness of deciduous crowns may make the placement of circumdental wires and arch bar slightly more difficult in children. • However the narrow cervix of tooth in relation to crown and roots provides better retention of wires as in Ivy loops or stout wires. • Mandibular cortex is thinner in children so care must be taken to avoid pulling a wire through the mandible when placing circummandibular wiring for splints
- 95. • While doing open reduction and fixation presence of tooth buds throughout the body of mandible must be a consideration as trauma to developing tooth buds may result in failure of eruption of permanent teeth and hence narrow alveolar ridge. • The emergency management of facial trauma in paediatric population also needs extra-consideration. • Clinical signs of shock may occur with even insignificant amounts of rapid blood loss due to small blood volume. • Because of small size of airway laryngeal edema or retroposition of base of tongue may produce sudden obstruction. • Tracheostomy if required should be done using vertical incision avoiding first tracheal ring and high lying left innominate vein.
- 97. When the arch bars cannot be placed due to traumatized or otherwise inadequate dentition, the fracture site can be immobilized with a lingual splint. The Risdon cable. A twisted 24-gauge wire is adapted to the cervical margins of the teeth across the dental arches and secured using interdental wires. This is a suitable alternative to arch bar placement in children and adolescents because its low profile is easier to adapt to the pediatric dentition.
- 98. Management of teeth in the fracture line • They are important in fracture stability when using IMF • They are less important in fracture stability when plates are used to fix the fractures. Reasons to extract the tooth • Severe tooth loosening with chronic periodontal disease and peri apical pathology • Partially erupted third molars with pericoronitis or cystic areas • Excessive delay from the time of fracture to the time of definitive treatment. • Fracture of the root of the tooth • Extensive periodontal injury and broken alveolar walls. • Displacement of teeth from their alveolar socket • Interference with bony reduction and reestablishing occlusion • Acute recurring abscess in the line of fracture despite antibiotic therapy
- 101. ETIOLOGY • Whenever a blow is received on the lateral side of face, the zygomatic arch protects the condyle and coronoid process. • Under these circumstances, the arch may fracture and may be associated with fracture or dislocation of the condyle • When a blow is given on the face resulting in fracture of the mandibular condyle, the position of the fractured condyle in relation to the remainder of the ramal stump will depend on certain factors: 1. The direction and degree of force. 2. The precise point of application of force. 3. Whether the teeth were in occlusion at the time of injury. 4. Whether the patient is partially or fully edentulous
- 102. MECHANISM OF INJURY Trauma Causing Condylar Injury, Lindahl 1977 Kinetic Energy imparted by moving object on static individual: Assault(fist) Industrial accidents Kinetic Energy derived from movement of individual and expended on a static object: Parade Ground Fracture - Fall of victim without attempt to shield face due to sudden loss of consciousness Fall during epileptic attack Kinetic energy summation of forces from combination of the above which produces more severe injury: RTA
- 103. Mechanism of injury to the condyles: (1) Blow, (2) Ground fall, (3) Dashboard RTA injury
- 104. CLASSIFICATION 1. Unilateral or Bilateral Fracture 2. Intracapsular(High Condylar) or Extracapsular (Low Condylar) fractures Intracapsular: Fractures involving articular surfaces, condylar neck just below articular surface Extracapsular: Fractures running deepest concavity of sigmoid notch to posterior direction
- 106. Other Classifications • Wassmund’s classification (1934) • MacLennan System (1952) - based on relationship of the proximal and distal fracture segments to each other • Spiessl and Scholl - based on displacement severity • Lindahl’s classification - considered comprehensive Requires radiograph taken in two planes at right angles to each other
- 107. LINDAHL CLASSIFICATION, 1977 1. ANATOMICAL LOCATION OF FRACTURE Condylar Head Condylar Neck Subcondylar 2. Relationship of the Condylar Fragment to the mandible Nondisplaced Deviated Displacement with medial or lateral overlap Displacement with anterior or lateral overlap No contact between fractured segments 3. Relationship of Condylar Head and Fossa Nondisplaced Deviated Dislocation
- 108. (A) Relationship of condylar fragment to mandible (B) Relationship of condylar fragment to glenoid fossa Anatomic Location of Fracture
- 109. • Fracture with little or no displacement occurs when adequate natural or artificial molar support exists and the teeth are in occlusion at the time of impact. • A variable degree of displacement will take place , if the teeth are separated or the force is received from a lateral direction. • Full force of impact will be transmitted to the condyles, resulting in a variable degree of fracture dislocation, if the mouth is widely open or there is inadequate molar support at the time of injury • When the blow is received in the center of the chin, the distribution of force is equal to both the condyles, -resulting in a bilateral indirect fracture through the necks, accompanied by a direct fracture at the symphysis (countercoup type of fractures). • This type more often is seen in an epileptic patients or soldiers who fall on the face during parade.
- 110. DIAGNOSIS 1. Evidence of facial trauma, especially in the area of the mandible and symphysis. 2. Localized pain and swelling in the region of the TMJ. 3. Limitation in mouth opening. 4. Deviation, upon opening, toward the involved side. 5. Posterior open bite on the contralateral side. 6. Shift of occlusion toward the ipsilateral side with possible cross bite. • Occlusion: Unilateral posterior crossbite or contralateral open bite (gagging of the occlusion on the ipsilateral molar teeth) and retrognathic occlusion may also be associated. Displacement of the condyle from the fossa or overriding of the fractured condylar neck shortens the ramus on that side producing the malocclusion.
- 111. 7. Blood in the external auditory canal. It is important to distinguish bleeding originating in the external auditory canal from the middle ear haemorrhage. The latter signifies a fracture of the petrous temporal bone 8. Pain on palpation over the fracture site 9. Lack of condylar movement upon palpation • If the condylar head is dislocated medially, a characteristic hollow over the region of the condylar head may occur 10. Difficulty in lateral excursions as well as protrusion 11. Persistent cerebrospinal fluid leak through the ear is indicative of an associated fracture of the middle cranial fossa (otorrhoea)
- 112. Bilateral Condylar Fracture 1. Signs and symptoms of unilateral condylar fractures present on both sides 2. Swelling over both fracture sites 3. Overall mandibular movement more restricted than in unilateral 4. Anterior open bite present if there is displacement of the condyles from glenoid fossa, or overriding of the fracture ends with posterior gagging of occlusion 5. Elongated face appearance 6. Pain and limitation on opening and restricted protrusion and lateral excursions 7. Frequent association with fracture of the symphysis or parasymphysis
- 113. Significant midline deviation towards the fracture side
- 114. Anterior Open Bite present in a bilateral condyle fracture Anterior and right lateral open bite associated with left mandibular condyle fracture
- 115. • Clinically, it will be noted that there is asymmetry of the face on the involved side due to, shifting of the mandible posteriorly and laterally towards the affected side (deviation of the mandible). • Premature occlusion on the involved side is caused by upward pull of the elevator muscles of the mandible. • An open bite deformity anteriorly and on the opposite side of the mandible is noted. In case of bilateral fracture condyles, the patient will have anterior open bite deformity with premature contact only on the posterior teeth. • This is caused by upward displacement of ramus and telescoping of the fractured fragments, due to contractions of the lateral pterygoid muscles
- 116. • In bilateral condylar fracture, which occurs below the attachment of the lateral pterygoid muscles, the patient is unable to protrude the mandible • In unilateral fractures at the same level, the patient is unable to perform lateral movements to the opposite side, as the lateral pterygoid muscle is out of function on the affected side • Fractures above the level of the lateral pterygoid muscle insertion do not exhibit displacement, as there is absence of contracting muscle attached to the proximal segment. • The patient may complain of severe pain in the TM joint and it will be noted that the teeth are separated and do not come into the occlusion on the affected side, because of the haemarthrosis in the joint, which forces the condyles downwards. • It may be few weeks before the teeth come into their normal occlusal relationship. • In this type of fractures, especially in children, active early mobilization of the joint is a must, the parents should be warned about the possibility of the development of ankylosis of the TMJ, if proper treatment is not initiated.
- 117. Radiology and Imaging • OPG-shows empty fossa and increase in joint space. • Reverse Towne’s view-showing elongated condylar fracture • PA mandible • CT scan(coronal)-important in sagittal fracture of the condyle.
- 119. Reverse Towne’s View
- 121. Goals of therapy 1. To get stable occlusion 2. Restoration of interincisal opening 3. Restore Full range of mandibular excursive movement 4. Decrease deviation 5. Eliminate pain 6. Avoid internal derangement 7. Avoid growth disturbance
- 122. TREATMENT OF CONDYLAR FRACTURES The management of condylar fractures is divided into: (a) Non-surgical - Conservative -Immobilization by Intermaxillary fixation Functional - Active movement (b) Surgical The decision will vary depending on the age of the patient, the type of fracture, concomitant injuries and associated anatomical findings.
- 123. Treatment of condylar fractures in infants and young children Unique anatomical features of infants condyle 1. Short thick necks with a less pronounced head. 2. Thin cortical bone with large marrow rich in undifferentiated pluripotent cells. 3. Trauma often leads to intra-capsular fractures. 4. Release of marrow and blood into the joint space readily predispose to ankylosis. Unless severely displaced, the fractures are treated by closed reduction with a short period of fixation not exceeding 10 days followed by mouth opening exercises to minimize the risk of ankylosis.
- 124. Treatment Protocol 0-2 years - Encouragement of active jaw function + analgesics 3-12years - Functional Treatment for both unilateral and bilateral condylar fractures. IMF for 7-10 days in case of extreme pain With significant displacement and ST injury, myofunctional interocclusal appliances may be used. 13-18years -Relatively decreased remodelling capacity. May result in abnormally shaped condylar head, shortened ramus heights. IMF for 2-3 weeks. Can be considered for surgery based on severity
- 125. In Adults: Unilateral Intracapsular Fracture Does not cause much deformity Conservative treatment (usual IMF for 7-10days) IMF for 2-3 weeks incase of malocclusion Bilateral Intracapsular Fracture IMF for 3-4weeks Physiotherapy afterwards to prevent restriction in mouth opening Unilateral Extracapsular Fracture No displacement, no disturbance to occlusion - no effective treatment Displacement or severe malocclusion - Open reduction Bilateral Extracapsular Fracture Results in instability and gross displacement of mandible Open reduction of at least one side is recommended to establish normal height If there is association with gross midfacial fractures, open reduction of both sides should be done
- 126. Nonsurgical Management of Condylar Fractures • Most cases of the condylar fractures are best managed through nonsurgical means. The obvious advantage is the avoidance of morbidity and complications associated with surgery. • Conservative method varies from no fixation to employing various devices. 1. Condylar fractures without displacement or with minimum displacement, without much occlusal disturbance and functional range of motion do not require any active treatment. • Patient is asked to restrict the movements and semisolid soft diet intake for 10 to 15 days followed by active movements.
- 127. 2. In case of deviation on mouth opening without much occlusal discrepancy, a simple muscle training in front of a mirror is adequate. On the involved side, class II elastic traction and on the normal side, vertical elastic forces may be beneficial. 3. In cases, where condylar fragment overriding is seen with alteration in ramus height, producing malocclusion, initially elastic traction is given to correct the malocclusion, followed by IMF for 2 to 3 weeks. • Early mobilization is advocated in cases of young children to avoid ankylosis of TMJ.
- 128. Surgical Correction of Condylar Fractures • Many a times, ankylosis, malocclusion, continued pain, dysfunction are examples of residual difficulties associated with the conservative management with condylar fractures Absolute Indications for Open Surgery 1. Fracture dislocations in the auditory canal or middle cranial fossa (rare) 2. Anterior dislocation with restricted mandibular movements 3. Bilateral condylar fractures associated with a comminuted LeFort III type with craniofacial dysjunction.
- 129. Zide and Kent indications for open reduction of condylar fractures Absolute indications: 1. Displacement of the condyle into the middle cranial fossa. 2. Inability to obtain adequate occlusion by closed techniques 3. Lateral extra-capsular dislocation of the condyle 4. Invasion by foreign body in the joint capsule
- 130. Relative Indications 1. Subcondylar fractures with overriding of the fragments with anterior open bite. 2. Anterior and medial displacement of the condylar fragment. 3. In case of delayed treatment, where there is pain and dysfunction associated with malunited fracture. 4. Unilateral or bilateral fractures with loss of the posterior teeth, in either upper jaw or both the jaws. 5. Cases in which position of the condylar fragment interferes with normal function of the jaws.
- 131. Surgical Approaches to the Condyle • Preauricular approach • Retromandibular approach • Submandibular approach • Intraoral approach • Bicoronal (bilateral condylar fracture along with frontal bone fracture)
- 133. Surgical Approach to the Condyle • The preauricular approach historically has had a relatively high incidence of facial nerve involvement. • Modifications of this approach include an approach to the joint region through a subtemporal fascial-periosteal envelope. Such an approach allows avoidance of the facial nerve branches by staying first posterior and then deep to the nerve. • Postramal approach is better for subcondylar fractures.
- 134. Methods of Fixation of the Condyle • Transosseous wiring • Kirschner wire • Intramedullary screw • Bone pins • Bone plating
- 135. Preparation of the patient • The temporal region is shaved preferably the day before surgery. • The skin of the preauricular region and the ear are prepared in the usual manner. • The patient should be placed on the table so that the sagittal plane of the head is parallel with the table. • This often requires that the shoulder be raised with a flat sandbag. Sandbags are also used to maintain the head in the correct position.
- 136. Operative Procedure • Operative procedure Access to the TMJ is done for high condylar fracture via modified preauricular incision and for subcondylar through postramal approach. • Blunt retractors are inserted and the zygomatic arch is located. The depression in the inferior border of the arch denotes the location of the mandibular joint. • The mandible at this point may be moved by the assistant, which may produce movement of the fragments and so helps in locating them. • As one proceeds, the transverse facial artery and vein may be encountered, cut and tied. Inverted L-shaped incision is taken from • the lower border of the zygomatic arch to the outer surface of the ramus.
- 137. • The procedure from here, depends on whether the condyle is displaced laterally or medially, which is already determined from the radiographs. • If the condyle is laterally displaced, then the periosteum of the neck of the condyle is stripped off with a periosteal elevator. • The condylar retractor is now inserted from the posterior border going medially to protect the vital structures. The hole is drilled through the outer cortex till the inner cortex. • The 26 gauge double wire is passed through the hole and grasped with the haemostat from the medial aspect
- 138. • The mandibular fragment is located next, since the fragment is under the condyle. If submandibular or postramal approach is taken, then small hole is made at the angle at the inferior border of the mandible, through which double wire is passed and grasped with a haemostat • This wire is pulled downward, so that there is better access for grasping the condylar fragment as well as ramus. • By using periosteal elevator and special condylar retractor, another hole is drilled in the ramal fragment. The wire, previously placed in the condylar fragment is now drawn through from the fracture surface by inserting a looped wire in the hole from the outer surface of the ramus.
- 139. • The fracture is then reduced under direct vision and temporary IMF is done intraorally by the assistant. • After that the wire ends are twisted together and cut off and the ends are bent over close to the bone. In cases, where condyles are medially displaced, the procedure is reversed. • First the mandibular fragment is located by manipulation and same procedure can be repeated as described. After fixation by the wires, the wound is closed in layers and dressing is given. • At the end of the operation, temporary IMF should be removed to facilitate extubation and it should be replaced next day. • Immobilization is kept for 15 to 20 days.
- 140. • Minibone plating can also be done instead of intraosseous wiring • Here, the fracture should be reduced as described and then the small four hole or two hole bone plate should be adapted to the external cortex and fixed with monocortical selftapping screws. • If the high condylar fractured fragment is displaced too anteromedially, then it should be located by depressing the ramal fragment and catching it with the haemostat. • Then if it can be fixed back as a free graft to the ramal stump, the attempt should be done. But many times condylectomy is recommended, because replantation is not possible.
- 143. Complications of condylar fractures 1. Permanent TMJ derangement e.g., osteoarthritis or internal joint derangement due to injury to the meniscus. 2. Facial asymmetry esp. in children due to growth interference. This may require osteotomy,bone grafting or distraction osteogenesis to correct the deformity. 3. Trismus 4. Ankylosis esp. following intra-capsular fracture in children. Shown in the radiograph as a mushrooming head of the affected condyle, also a prominent antegonion notch. 5. Lateral open bite.
- 144. Early/concurrent complications 1. Fracture of the tympanic plate 2. Fracture of the glenoid fossa with or without displacement of the condylar segment into the middle cranial fossa. 3. Damage to the trigeminal and facial nerves 4. Vascular injury 5. infection
- 145. Late complications • Delayed union • Non-union • Malunion • Malocclusion • Growth disturbances • Tmj dysfunction • Ankylosis • Scars
- 146. References. • Oral & maxillofacial trauma- Fonseca,vol 1 • Maxillofacial Injuries- Rowe & Williams • Textbook of oral & maxillofacial surgery by SM Balaji • Textbook of oral & maxillofacial surgery by Peter Ward Booth. • Textbook of oral & maxillofacial surgery by Neelima malik. • Killeys - fractures of the mandible
- 147. THE END!!