Keratoconus is a non-inflammatory thinning and bulging of the cornea that results in irregular astigmatism. It typically develops during adolescence or early adulthood. While the exact cause is unknown, genetic and environmental factors likely play a role. Early stages are often managed with glasses or rigid gas permeable contact lenses, which provide a regular surface. Close monitoring is needed as the condition may progress, requiring consideration of surgical options like corneal transplantation if contact lenses become intolerable or vision deteriorates.
![Introduction to Keratoconus
Keratoconus, conical cornea, is an interesting, complex, and challenging
condition for both the patient and contact lens practitioner alike.
The aetiology of keratoconus is still not well understood, but it would
seem to include both genetic and environmental factors. Around the
second decade of life (between 12 and 20 but cases have been reported
at birth and as late as 51 years of age [Heverly and Lowther, 2005]),
the cornea of a keratoconic patient begins to thin and protrude,
producing irregular corneal astigmatism.
Despite our ability to detect and document keratoconus, especially in the
era of videokeratoscopy, there is still no early treatment or cure, and
individual prognosis is highly variable . Optimal treatment depends on
the severity of the disease process, requires accurate diagnosis, and
may require the use of a number of therapeutic alternatives.](https://image.slidesharecdn.com/2-keratoconusandcontactlenses-180528154238/75/Keratoconus-and-Contact-lenses-2-2048.jpg)
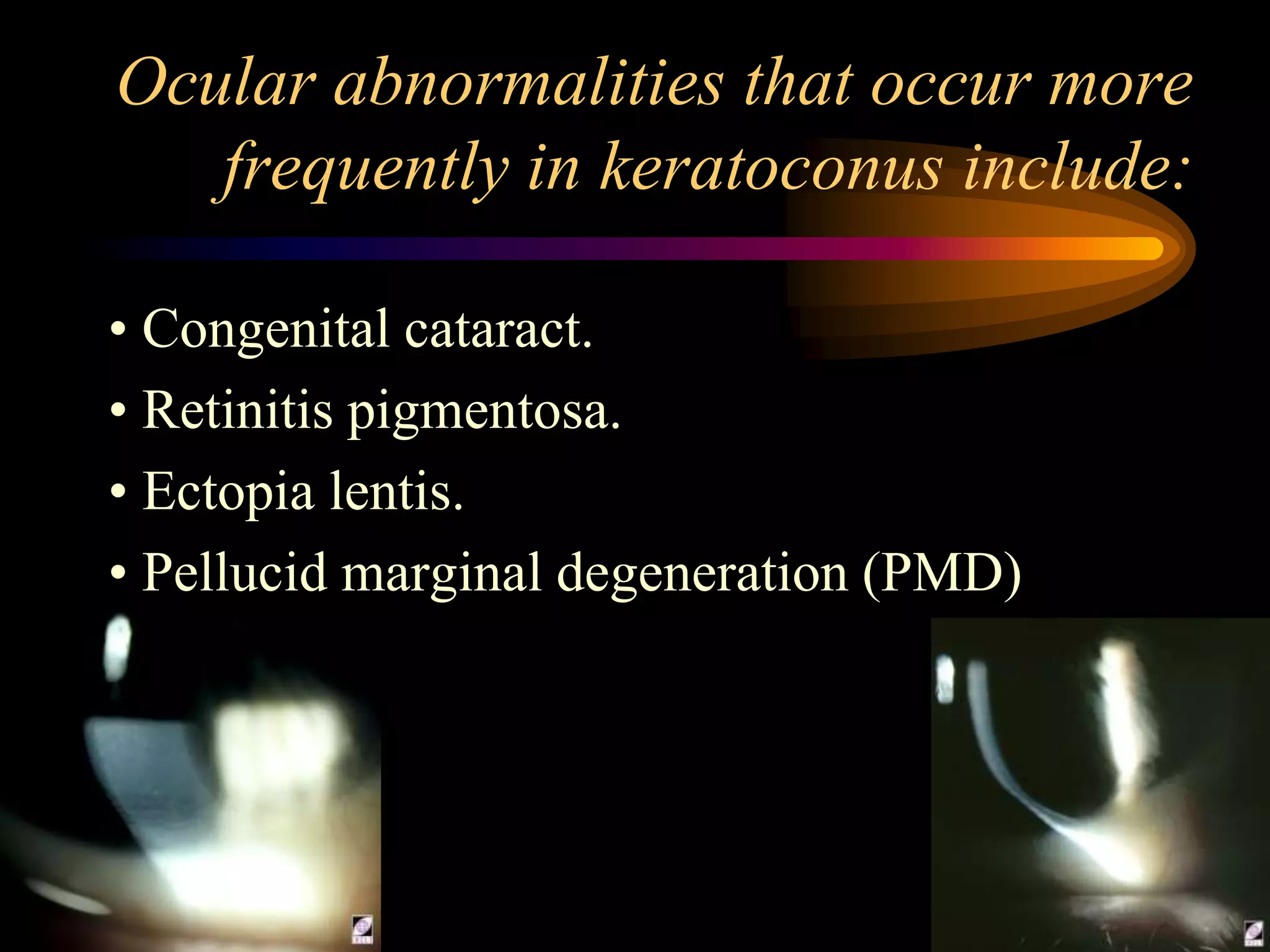
![If the progress of the disease is marked by the
following issues, surgical options may have to be
considered:
1. Increased RGP lens intolerance.
2. The development of stromal opacities.
3. Corneal hydrops.
4. Significant lens decentration and/or an inability to
retain lenses on the eyes.
5. Increased astigmatism/irregular astigmatism.
Keratoconus is a leading indication for corneal
transplantation (Penetrating Keratoplasty [PK]). The
reasons for performing a PK according to several
sources appear in descending order.](https://image.slidesharecdn.com/2-keratoconusandcontactlenses-180528154238/75/Keratoconus-and-Contact-lenses-4-2048.jpg)



![Cont.
The protrusion usually develops in the infero-
central zone of the cornea that results in a
cone-like anterior protrusion exhibiting a high
degree of irregular, myopic astigmatism, and
marked visual impairment (data in slide 7 comes from the
Collaborative Longitudinal Evaluation of Keratoconus Study [CLEK]).
The condition typically, though not always,
affects young people in the second or third
decades of their lives.](https://image.slidesharecdn.com/2-keratoconusandcontactlenses-180528154238/75/Keratoconus-and-Contact-lenses-8-2048.jpg)