Objectives
• Understand dailyfluid and electrolyte
requirements for an average adult
• Understand the major components of
replacement fluid
• Maintenance versus Resuscitation
• Complications of fluid therapy
4.
Input and Output
ofthe “Normal” Adult
• Minimal Obligatory Daily input:
– Ingested water: 500mL
– Water content in food: 800mL
– Water from oxidation : 300mL
» TOTAL: 1600mL
• Minimal Obligatory Daily water output:
– Urine: 500mL
– Skin: 500mL
– Respiratory tract: 400mL
– Stool: 200mL
» TOTAL: 1600ml
On average, an adult input and output is 30-35mL/kg/day (about
2.4L/day)
Maintenance Therapy
• Replacesthe ongoing losses of water and
electrolytes under NORMAL physiological conditions.
• Used when the patient is not expected to eat or
drink normally for prolonged period of time.
• Patients who are afebrile, not eating, not physically
active require less that 1 L of electrolyte free water
per day.
8.
Fluid Resucitation
• Correctexisting abnormalities in volume status or
serum electrolytes
• Parameters used to assess volume deficit:
– Blood pressure
– Jugular venous pressure
– Urine sodium concentration
– Urine output
– Pre and post deficit body weight
9.
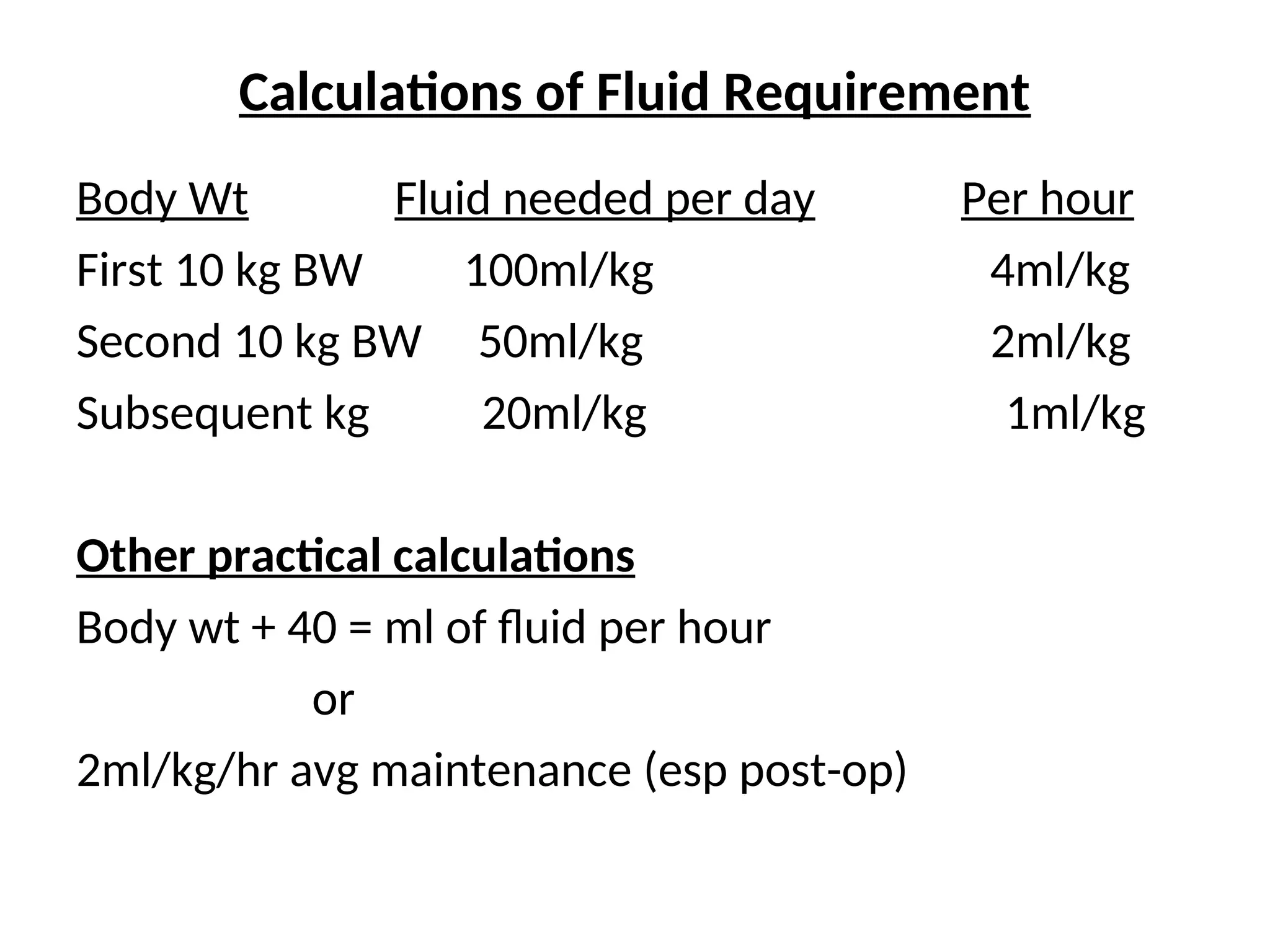
Calculations of FluidRequirement
Body Wt Fluid needed per day Per hour
First 10 kg BW 100ml/kg 4ml/kg
Second 10 kg BW 50ml/kg 2ml/kg
Subsequent kg 20ml/kg 1ml/kg
Other practical calculations
Body wt + 40 = ml of fluid per hour
or
2ml/kg/hr avg maintenance (esp post-op)
10.
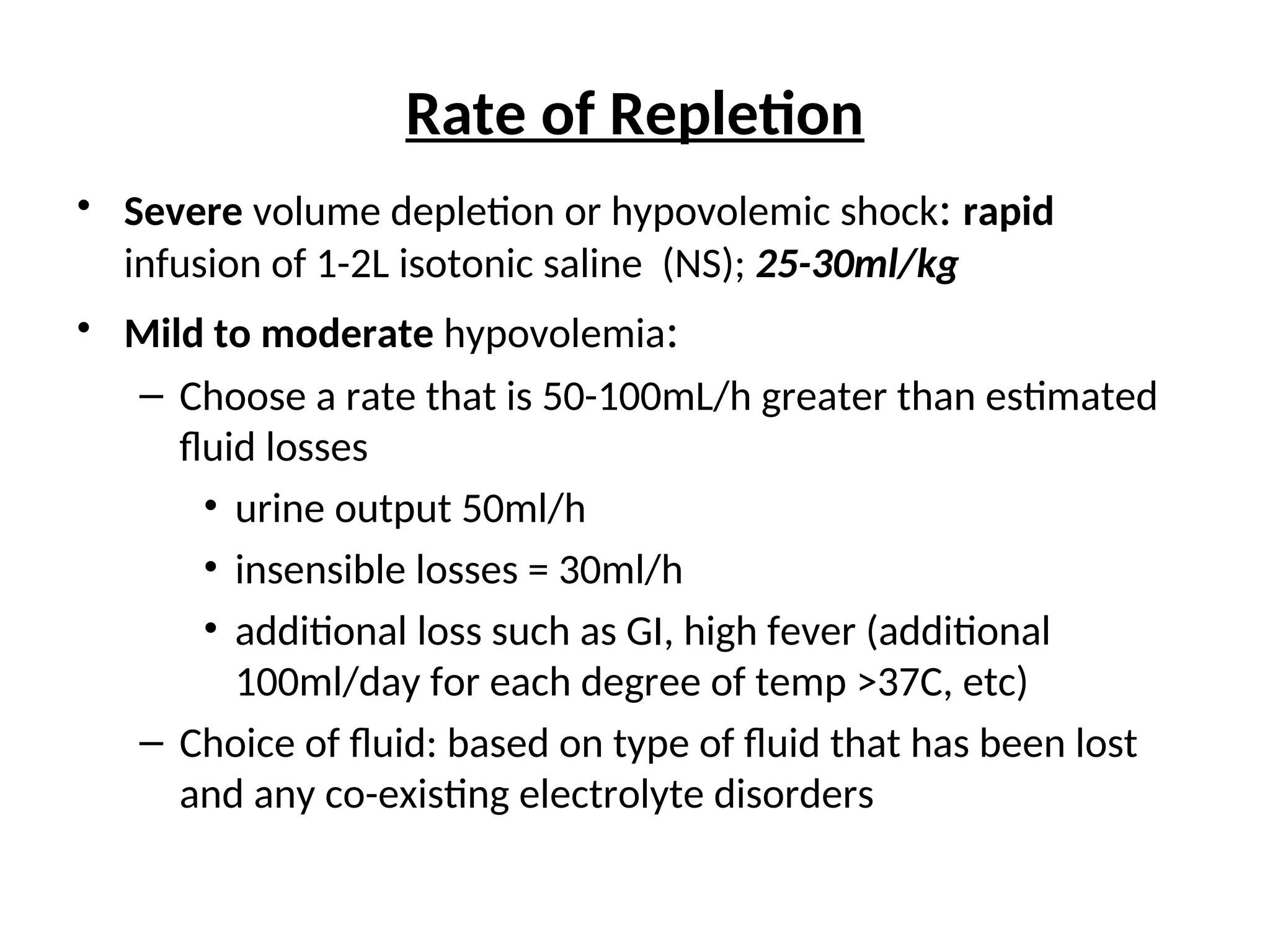
Rate of Repletion
•Severe volume depletion or hypovolemic shock: rapid
infusion of 1-2L isotonic saline (NS); 25-30ml/kg
• Mild to moderate hypovolemia:
– Choose a rate that is 50-100mL/h greater than estimated
fluid losses
• urine output 50ml/h
• insensible losses = 30ml/h
• additional loss such as GI, high fever (additional
100ml/day for each degree of temp >37C, etc)
– Choice of fluid: based on type of fluid that has been lost
and any co-existing electrolyte disorders
11.
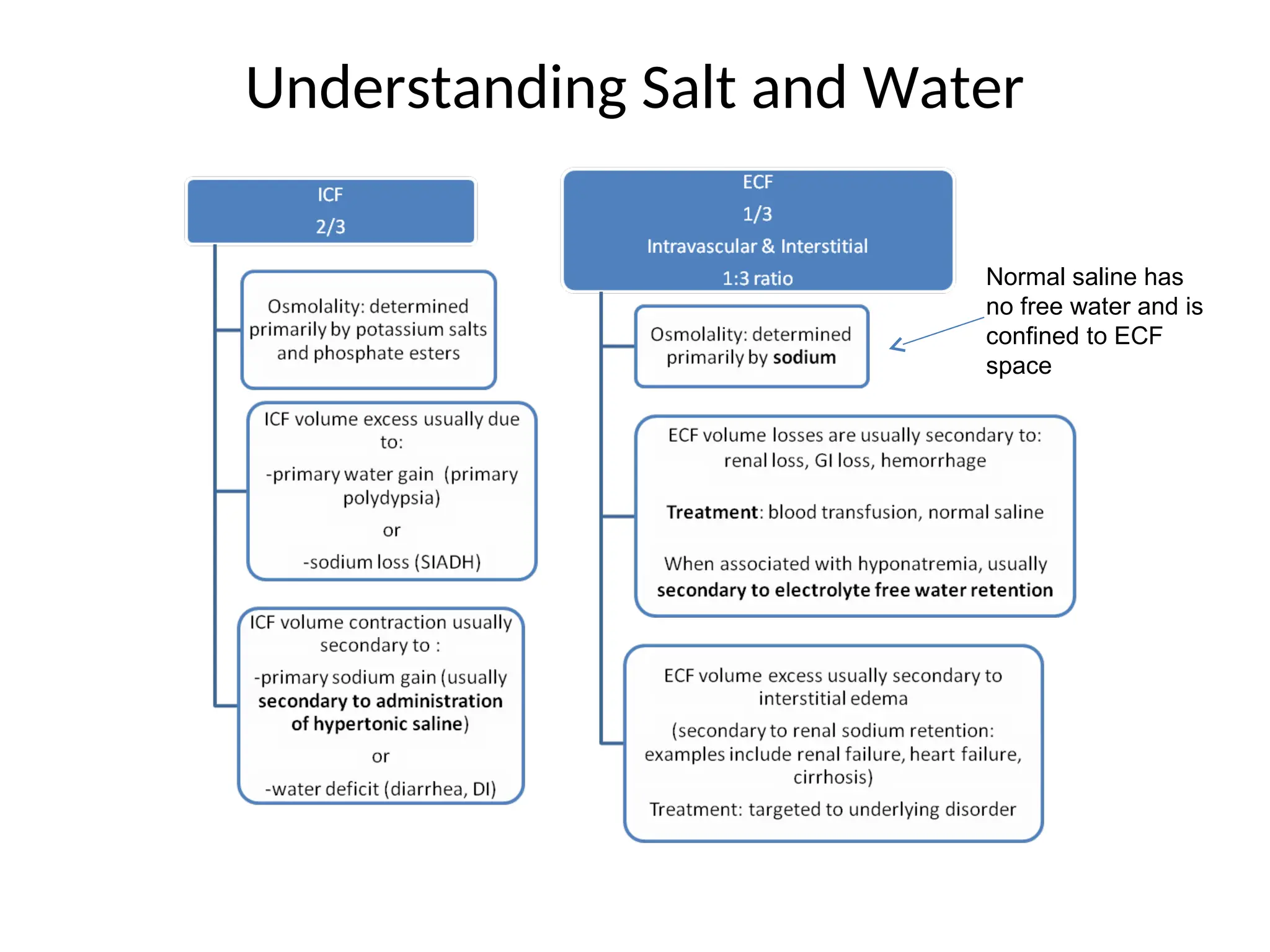
Understanding Salt andWater
Normal saline has
no free water and is
confined to ECF
space
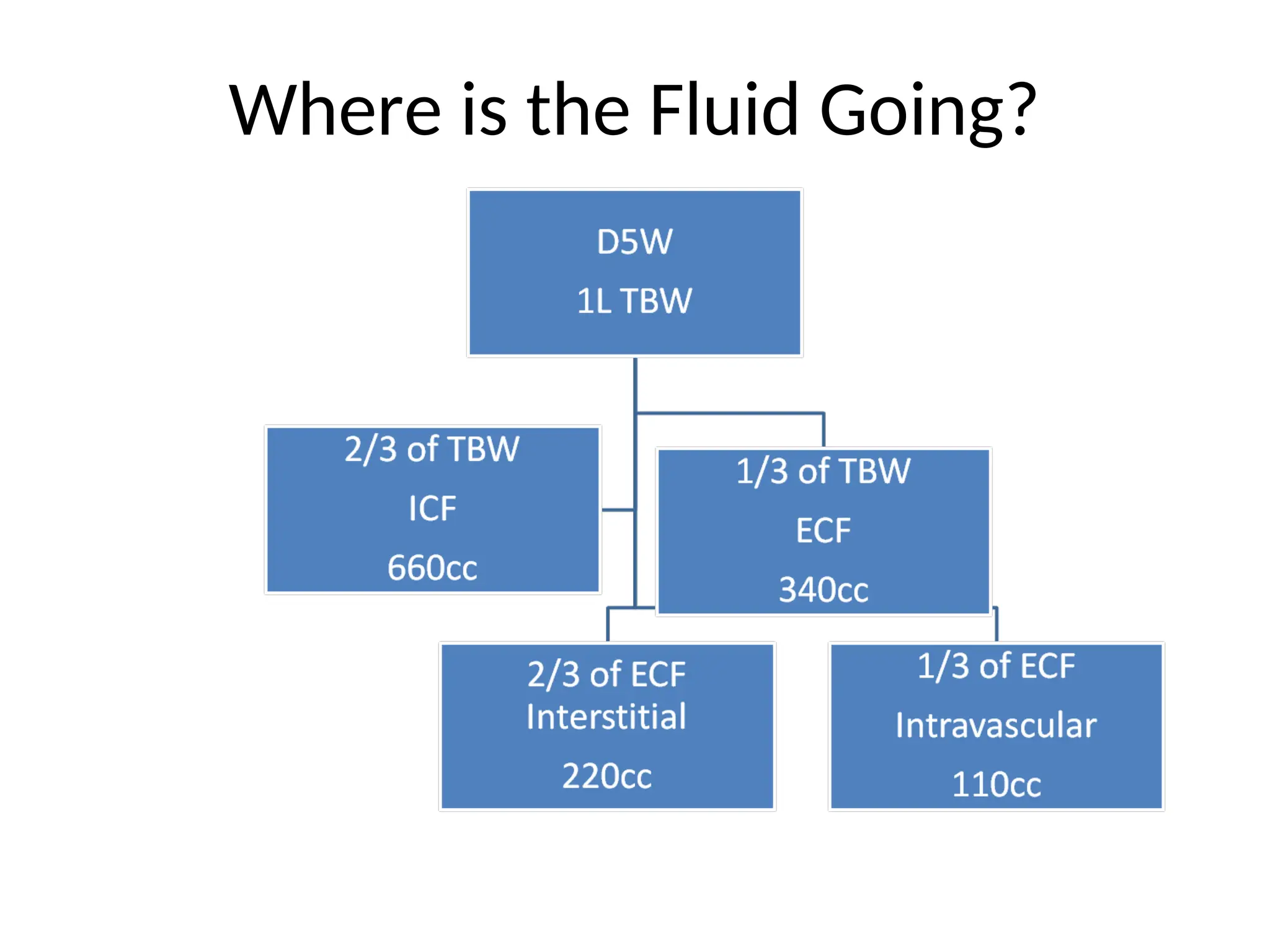
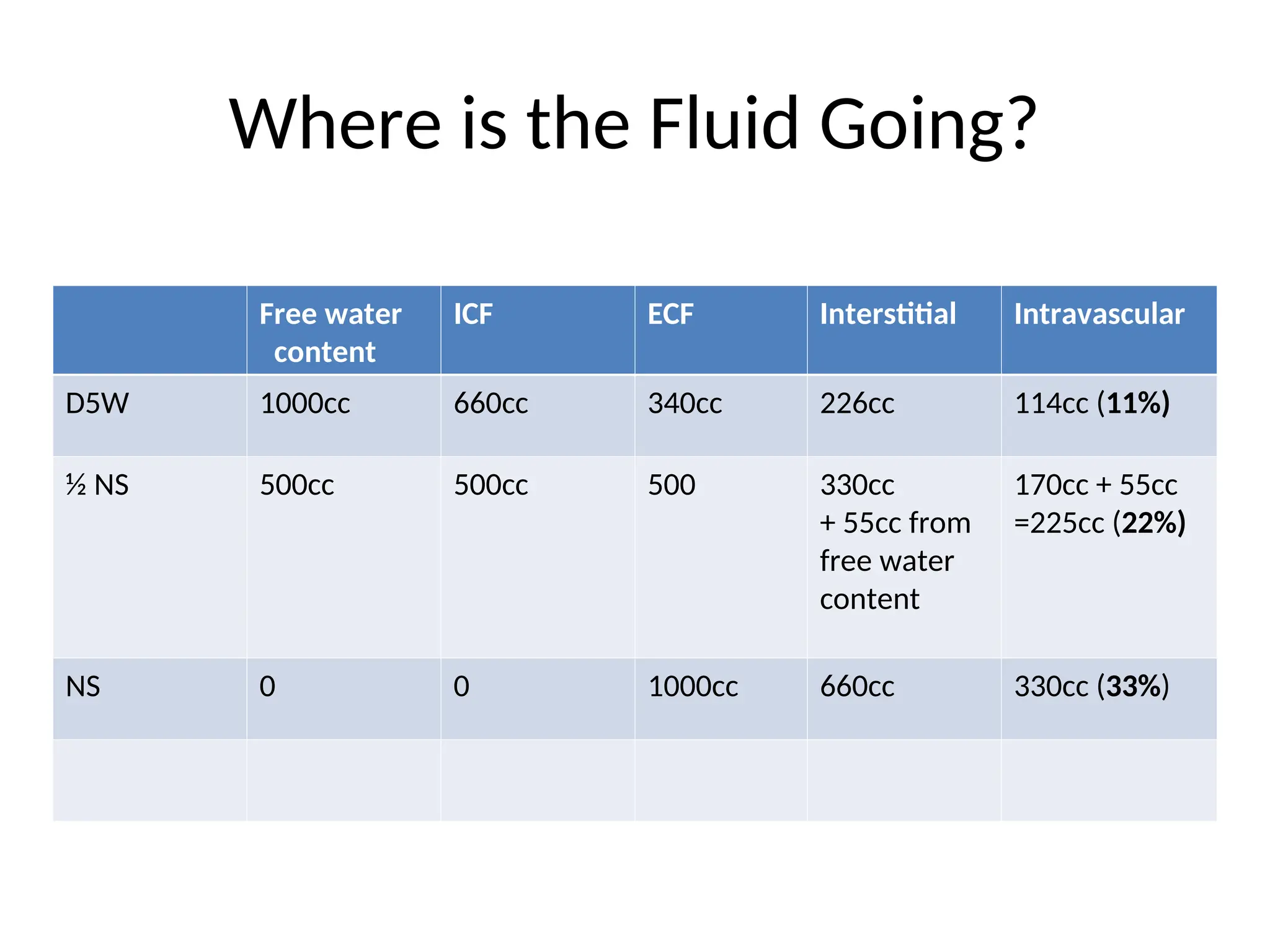
Where is theFluid Going?
Free water
content
ICF ECF Interstitial Intravascular
D5W 1000cc 660cc 340cc 226cc 114cc (11%)
½ NS 500cc 500cc 500 330cc
+ 55cc from
free water
content
170cc + 55cc
=225cc (22%)
NS 0 0 1000cc 660cc 330cc (33%)
14.
Crystalloids
• A solutionof small and low molecular wt particles.
• Solutes (MW<30,000) either ionic (Na+ , Cl-) or non-
ionic (e.g mannitol).
• Osmotic pressure zero
• Pass freely across the microvascular membrane.
• Inexpensive
Uses of HypotonicCrystalloid Solutions
• Fluid loss & dehydration
• Hypernatremia
• Gastric fluid loss
• Cellular dehydration from excessive diuresis
• Slow rehydration
17.
Isotonic Crystalloid Solutions
•e.g. Ringer’s solution, 0.9% normal saline
Uses of Normal Saline Uses of Lactated Ringers
• Shock Dehydration
• Resuscitation Burns
• Fluid challenges (?assess) GI tract fluid loss
• Blood transfusions Acute blood loss
• Hyponatrenia Hypovolemia
• DKA
18.
Hypertonic Crystalloid Solutions
•e.g. DNS, 3% Saline
• Used in:
Heat related disorders
Fresh water drowning
Correction of severe hyponatremia (3% NaCl)
19.
Adverse effects oflarge volume crystalloid infusion
• Extravascular accumulation in tissues like skin,
connective tissue & lungs.
• Inhibition of gastrointestinal motility due to gut
edema.
• Delayed healing of anastomosis.
• Saline-induced hyperchloremic acidosis.
20.
Colloids
• High molecularwt substance.
• Largely remains in the intravascular compartment;
Generates oncotic pressure.
• e.g., human albumin, gelatins & dextrans.
• Molecular wt of a colloid directly influences its
intravascular persistence. Gelatins have smallest MW
and HES the highest.
• HES solutions have highest MW.
21.
Human Albumin Solutions
•Contributesto 80% of normal oncotic pressure.
Hydroxyethyl Starch Solutions (Heta/Pentastarch)
•Starches derived from glycopectins & modified by
addition of hydroxyethyl groups.
•Increase in colloid osmotic pressure with HES equal to
that with albumin.
Gelatin solutions
•Derived from bovine collagen.
•Low MW substances
22.
Summary
• Treat IVfluids as “prescription” like any other medication
• Determine if patient needs maintenance or resuscitation
• Choose fluid type based on co-existing electrolyte
disturbances
• Don’t forget about additional IV medications patient is
receiving
• Choose rate of fluid administration based on weight and
minimal daily requirements
• Avoid fluids in patients with ECF volume excess
• Always reassess whether the patient continues to require IVF
Editor's Notes
#4 Emphasize the minimal intake/output of an average daily adult in order to understand rate and goal of fluid administration we order for our patients
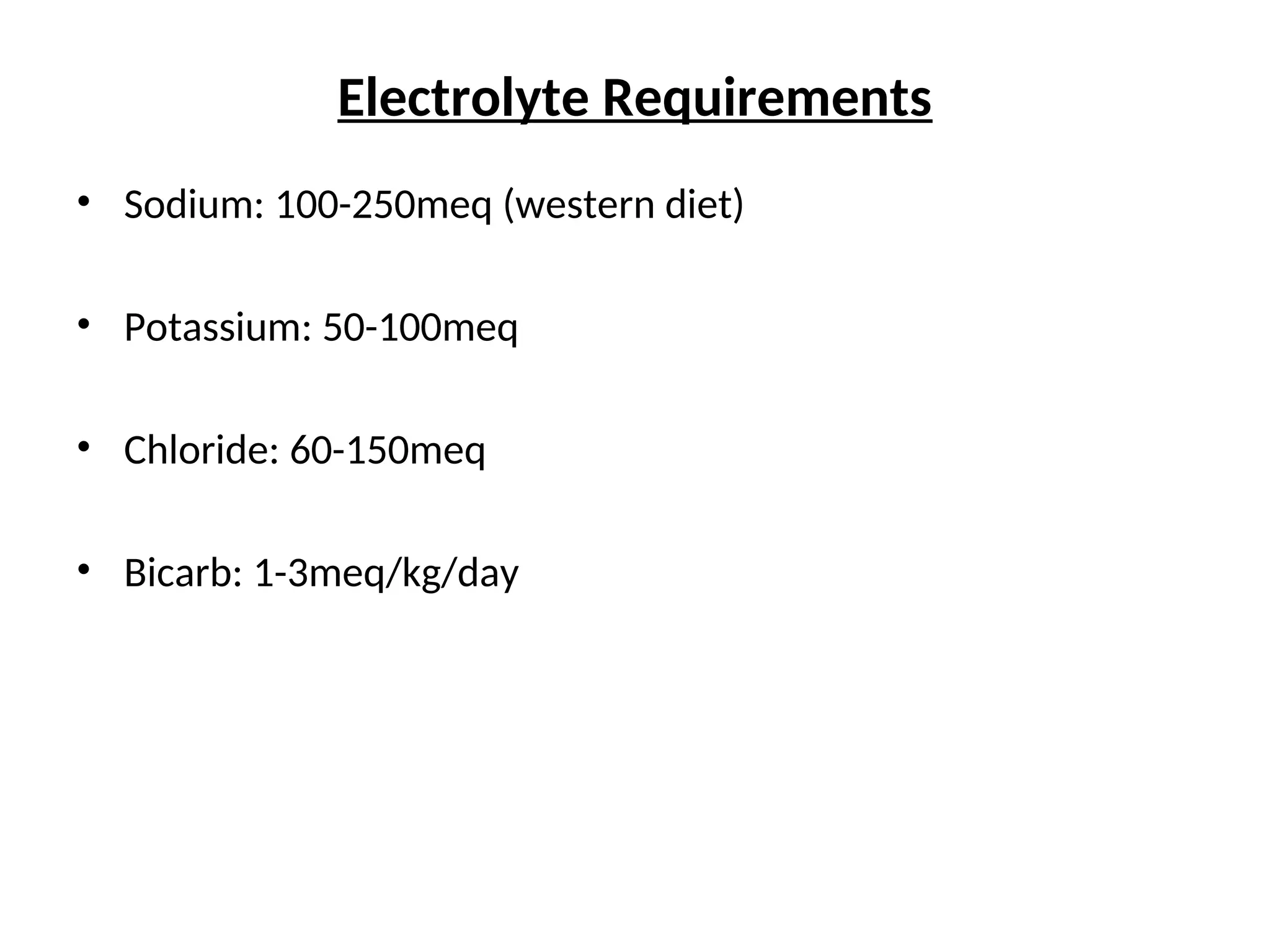
#5 No need to memorize, just to understand where the content of electrolytes in different fluid solutions comes from
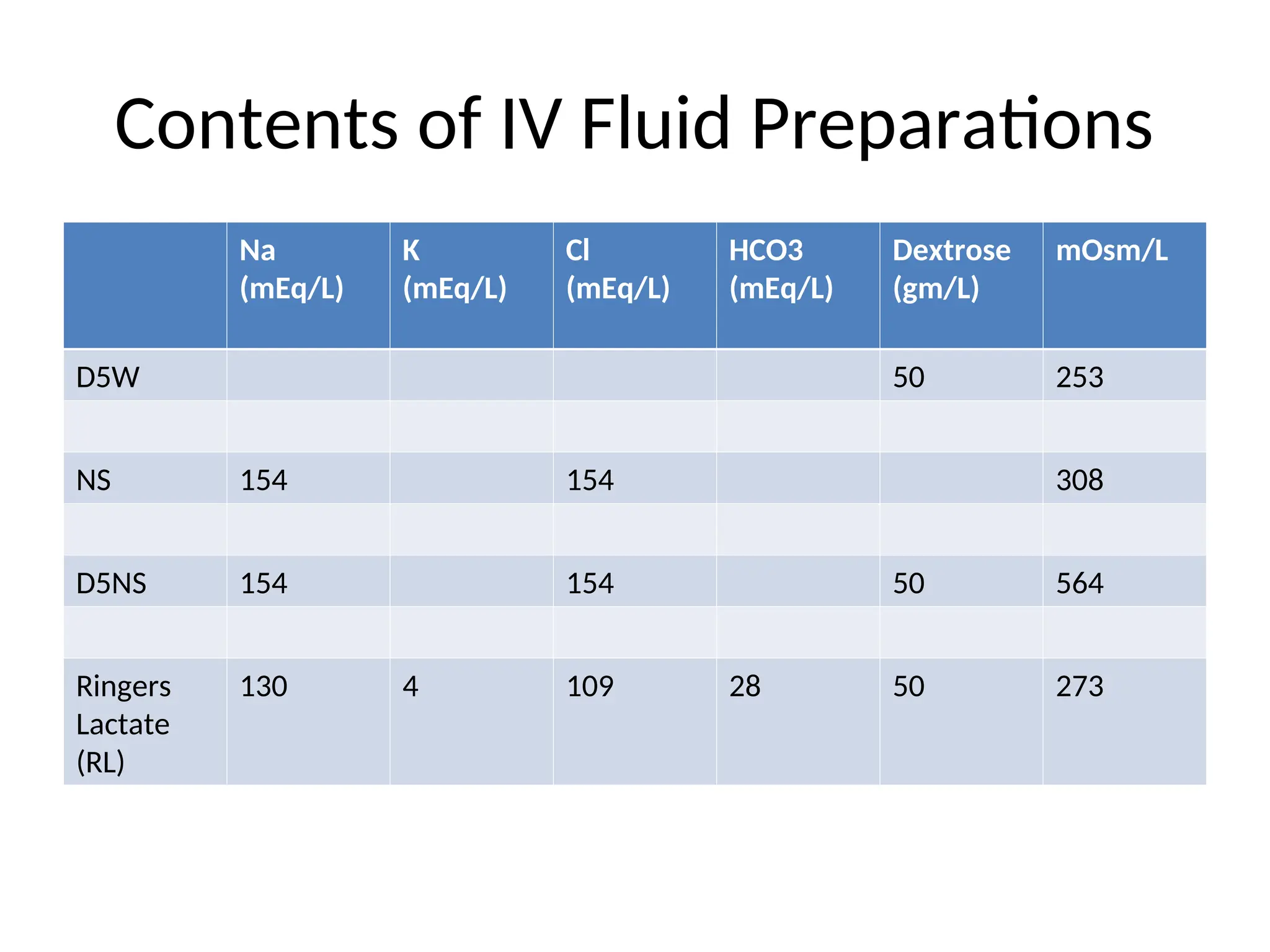
#6 Important to understand the differences between the types of fluid we administer and the osmolality of each solution. Recognize that although D5 appears isotonic, the dextrose is metabolized quickly and therefore becomes a hypotonic solution rather rapidly.
#8 Transition from fluid administration for purpose of maintenance therapy to recognizing when fluids are being given for the purpose of resuscitation. Have the team come up with answers regarding the parameters used to assess volume deficit.
#10 Think about minimal intake/output and add 50-100ml/hr based on additional losses for each patient
Fluid of choice is generally normal saline. Lactate Ringer’s will be used in primarily in cases where you are trying to prevent re-expansion acidosis (as in acute pancreatitis).
#11 Not meant to be memorized. Just to remind ourselves the different components of free water in our body, and how sodium and volume excess/loss effects each compartment.
#12 To understand what happens to the IV fluids we give our patients- recognize that if D5W is given, only 10% of it will end up in the intravascular space. This is the reason we don’t give D5W for resuscitation.
#13 Compare each type of commonly administered fluid and recognize how much stays in the intravascular space versus ICF and interstitial. Target therapy to your goal of expansion in each compartment.