1) Successful endodontic therapy requires thorough cleaning and disinfection of the root canal system to eliminate bacteria.
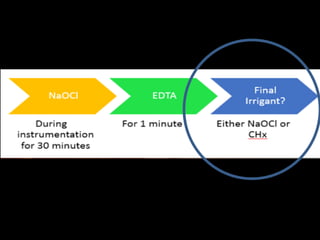
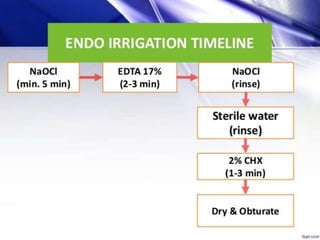
2) No single irrigant can achieve all the desired properties of dissolving tissue, disinfecting, and removing smear layer. The sequential use of sodium hypochlorite, EDTA, and chlorhexidine helps achieve through cleaning.
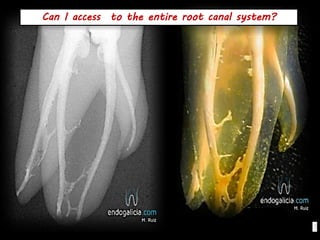
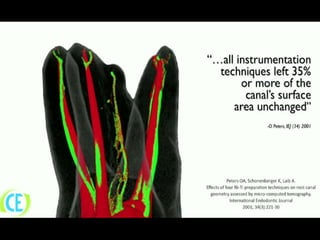
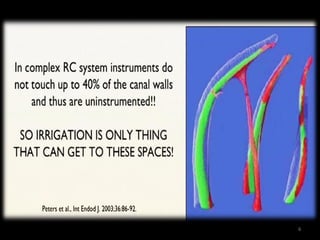
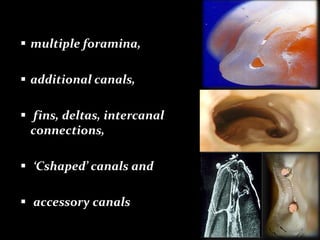
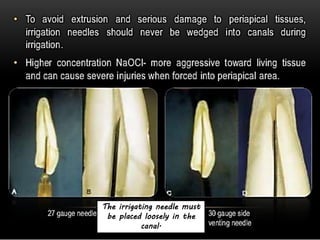
3) Proper irrigation technique, including using small-gauge needles, up and down motion, and replenishing irrigants, is important for disinfecting inaccessible areas of the complex root canal anatomy.