1. Dr. Milan Kharel presented on inhalational anesthetic agents and provided a history of anesthesia including the first use of diethyl ether and chloroform.
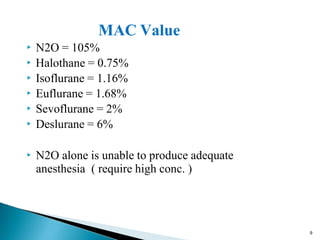
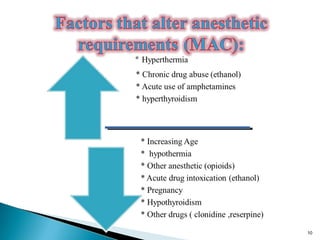
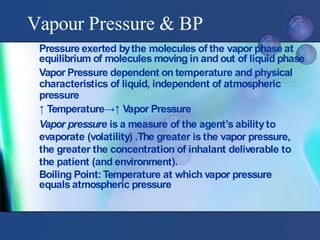
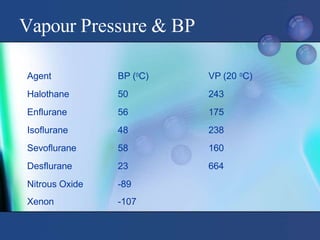
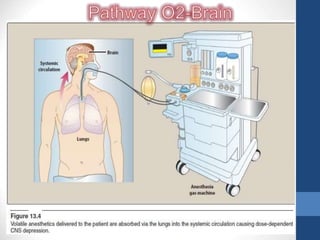
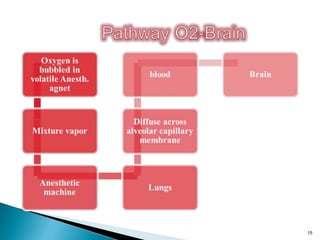
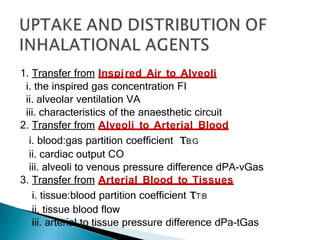
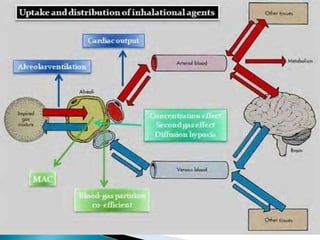
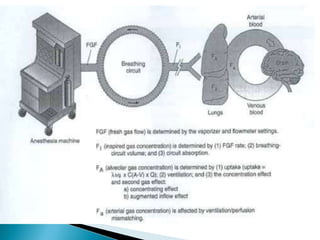
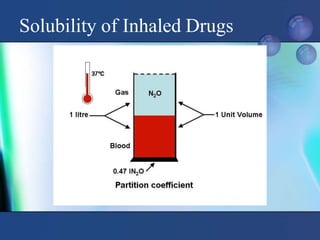
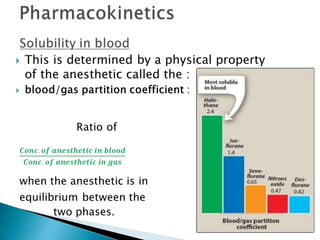
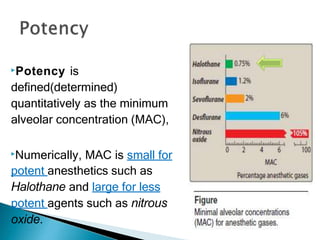
2. Key concepts around MAC, vapor pressure, blood solubility, and the three stages of gas transfer from inspired air to tissues were discussed.
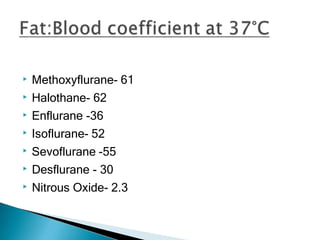
3. Ideal properties of anesthetic agents include rapid induction and recovery, precise control of anesthetic depth, and an absence of toxic effects. Nitrous oxide, halothane, isoflurane, sevoflurane, and desflurane were compared based on their solubility and other characteristics.


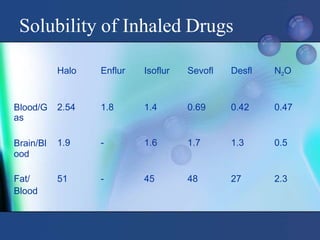




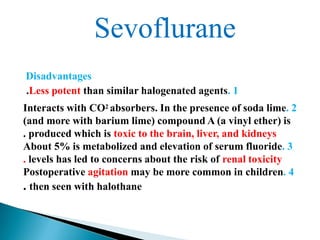
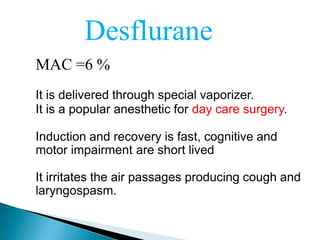
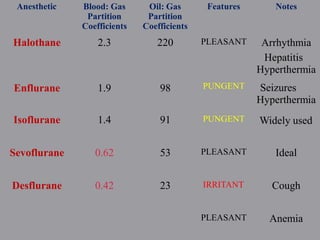






















































![PHYSIOLOGY OF LABOUR PAIN AND LABOUR ANALGESIA [Autosaved] [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/physiologyoflabourpainandlabouranalgesiaautosavedautosaved-230406110245-4cf32dcd-thumbnail.jpg?width=640&height=640&fit=bounds)






















