The document provides information about various anatomical structures and injuries related to the lower limb. It describes:
1. The muscles present after cutting the gluteus maximus, including their nerve supply and actions on the hip joint.
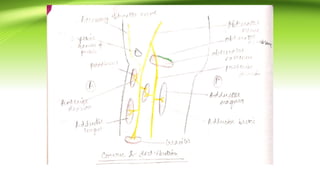
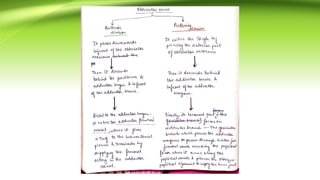
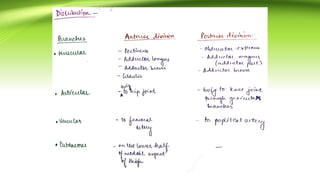
2. The nerves involved in an injury where a person lost adduction of the leg after an automobile accident, including the origin, branches, and distribution of the injured nerve.
3. Details about the semilunar cartilages of the knee joint, which are prone to injury from twisting strains, along with the anatomical basis of and notes on an injury where a footballer sustained a sprain and difficulty moving the left knee after kicking with his right foot.