
Recommended
More Related Content
Similar to Slide Presentation on Endocarditis .pptx
Similar to Slide Presentation on Endocarditis .pptx (20)
Recently uploaded
Recently uploaded (20)
Slide Presentation on Endocarditis .pptx
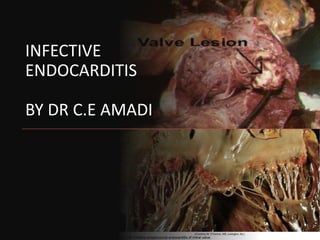
- 1. INFECTIVE ENDOCARDITIS BY DR C.E AMADI
- 3. A 28- year old man with a medical history of mitral regurgitation presented at the ER after an episode of transient weakness in his right arm and slurred speech. He under went dental scaling a month earlier. He in addition has recurrent history of fevers, general malaise and weight loss. On cardiac exam he has anaemia, finger clubbing and unchanged intensity of the MR. Echocardiography shows a mobile 1.2cm mitral valve vegetation and moderately severe MR
- 4. Cont’d A 45 year old Nurse with background history of CHF had prosthetic mitral valve replacement 11 months ago. She presented at the Cardiology OPD with 3 weeks history of fever, worsening symptoms of heart failure and chest infection. Cardiac exam showed increased intensity of the MR while echo showed partial dehiscence of the prosthetic valve, para-valvar turbulent flow and mobile vegetation along the valve commissures
- 5. Cont’d A 45 year old man with advanced NHL was admitted for chemotherapy. 48 hours later he developed high grade fever and mitral regurgitation. Echocardiography showed hyperechoic masses on the anterior mitral valve leaflets and moderate MR Blood culture showed pure isolates of Staph aureus
- 6. DEFINITION • A infection of the endocardial surfaces of the heart which may include • One or more valves ( native or prosthetic) • mural endocardium • Septal defects • Endothelial surfaces of the great arteries.
- 7. Also includes infection of intravascular lines/implants such as central lines, dialysis catheters, pacemaker leads , intra-cardiac devices Infections of patent ductus arterious and coarctation also constitute IE The infection is usually bacteria but occasionally fungi, mycoplasma, chlamydia may be involved
- 8. Usually causes severe valvar damage and incompetence, heart failure and extra-cardiac complications. Usually fatal if not properly treated
- 9. History of IE 1674 In 1674, Lazaire Rivere first described the gross autopsy findings of IE in this work Opera medica 1885 In1885 William Osler presented the first comprehensive description on IE in English 1966 The first scientific publication of IE was in the New England Journal of Medicine in 1966 by Lerner and Weinstein
- 10. Classification Native valve IE (Acute or Sub acute) Prosthetic Valve IE (Early or Late) Intravenous Drug Abuse ( IVDA) IE Nosocomial Hospital Associated IE
- 11. Native Valve IE Usually constitutes about 50-60% of cases of IE Affects natural valves Two types viz Acute and Sub-acute
- 12. Acute NVIE usually affects normal valves in debilitated people Usually no associated structural heart disease Has an aggressive course leading to valve destruction and embolic complications especially stroke Fatal under 6 wks if not treated Typical causative organism: Staph aureus Group B Strep
- 13. Sub-acute NVIE usually affects abnormal or damaged valves There may be associated congenital heart diseases (repaired or unrepaired) e.g. PDA, VSD, TOF , MVP Degenerative heart diseases such as Marfan’s syndrome, Aortic stenosis
- 14. Usually runs an indolent cause Metastatic infection is rare Fatal if not treated under 1 yr Typical organisms are Strept viridans viz bovis, sanguis, mitis; Enterococci Coagulase negative Staph aureus Gram -ve bacilli
- 16. Prosthetic Valve IE PVIE accounts for 10-20% of IE Mechanical valves more at risk within 3 months of surgery; Mitral valves more at risk than aortic valves Two types viz Early and PVIE
- 17. Early PVIE occurs within 12 months of valve replacement Usually caused by Coagulase –ve Staph(Staph epidermidis), Gram –ve bacilli and Staph aureus Usually due to contamination at the time of surgery
- 18. Late PVIE occurs more one yr following valve implantation Usually community acquired Typical microbes include Streptococci, Enterococci Staph aureus Recent data suggest that Staph aureus is often implicated in both early and late PVIE
- 19. Early PVE is commoner than late PVE Mechanical valves are at higher risk than bio-prosthetic (tissue) valves within the first yr; Risk higher for bio-prosthetic valves after 1 year Risk comparable after 5 yrs of valve replacement
- 20. Intravenous Drug Abuse IE Common in i.v drug abusers and HIV patients About 75% of patients do not have any structural heart disease The tricuspid valve is affected in about 60% of cases, aorta (25%), mitral(5%); mixed (5%) Aortic or mitral valve may be affected
- 21. IVDA IE Staph aureus is the most common causative agent(50%); Pseudomonas, Candida, Streptococci Enterococci HACEK group of bacteria
- 22. HACEK are Gram negative fastidious slow growing bacteria. Haemophilus parainfluenza Actinobacillus actinomycetecomitans Cardiobacterium hominis Eikenella corrodens Kingella kingae Commensals of upper airway and oropharnyx
- 23. Nosocomial IE Also called Healthcare Associated endocarditis Usually manifests 48 hrs following admission or associated with a hospital based procedure e.g. central lines, dialysis shunts/catheters Commonly caused by Staph aureus, and enterococci
- 24. Two types of NIE viz Right sided NIE caused by injury due a normal valve during vascular procedures Left sided NIE from a previously damaged valve
- 25. Epidemiology Incidence varies globally; 2-4 cases/100,000 to 15-30/100,000 depending on the age and prevalence of i.v drug abuse Males are 3X more affected than females No racial predilection
- 26. Depends on age and region Younger age group: Congenital heart diseases & repair in developed countries; Rheumatic heart dx primarily and congential heart disease/repair in developing countries
- 27. Older age group: Degenerative heart Dx, IVDA, increased use of invasive procedures in developed countries; Increasing use of intra-cardiac devices , prosthetic valves and degenerative heart Dx in the developing countries
- 28. Valvular Distribution of IE Mitral 28-45% Aortic 5-36% Both 0-35% Tricuspid 0-6% Pulmonary < 1%
- 29. Predisposing Factors • Age • DM • Immunosuppression • HIV • Long term dialysis • Poor dental hygiene • Previous IE • Use of intravascular lines/catheters • Rheumatic disease • Valve repairs/replacement
- 30. Aetiopathogenesis of IE Prerequisite for IE; Damaged endothelium Bacteraemia Host Factors Virulence and Inoculum of the organism
- 31. Aetiopathogenesis Cont’d Damaged endothelium viz: Disease e.g RHDx, Intravascular procedures Flow from high pressure to low pressure chamber Flow across a narrow orifice at high velocity Repeated injection of solid particles in IVDA
- 32. Aetiopathogenesis Cont’d Bacteraemia : Poor dental hygiene IVDA Soft tissue injuries Genito-urinary procedures Colonic procedures Procedures on septic loci
- 33. Etiopathogenesis Cont’d Host Factors(Immunity) viz: Local Systemic Virulence and inoculum of the Organism
- 34. Pathophysiology Normal endocardium Laminar blood flow Resistant to bacteria colonization Damaged endocardium Turbulent blood flow with eddy current (Venturi effect) Easily colonised by bacteria Hypercoaguable state usually results
- 35. Pathophysiology Cont’d Promotes platelet & fibrin deposition leading to formation of sterile vegetation( Non-Bacterial Thrombotic Endocarditis) In the event of sufficient virulent bacteraemia and poor host factors bacteria adhere to the platelet and fibrin rich NBTE This complex is called vegetation, the pathologic hallmark of IE
- 36. Complications of vegetation Cardiac Valve destruction & haemodynamic changes Infection may extend to paravalvular tissue leading to mural abscess Large vegetations may cause functional stenosis Cardiac failure Arrhythmias Pericarditis
- 37. Embolic/Metastatic (Large, mobile, mitral, Staph) Lung abscess Septic arthritis Splenic infarction Renal abscess/renal failure from AGN Cerebral abscess, spinal abscess, Stroke Osteomyelitis Mycotic aneurysm
- 38. Microbiology of IE Staph aureus (40%) Strept viridans (34% Enterococci (6%) Coagulase –ve Staph aureus (5%) Gram –ve bacilli (6%) Fungi (2%) HACEK group/Polymicrobe (3%) Culture negative IE (4%)
- 39. Clinical features Fever & chills are the most common symptoms (80%) Constitutional symptoms: Malaise Weight loss Anorexia Arthralgia Headaches Night sweats Cough Shortness of breathe Chest pain Abd pains
- 40. Features of CHF Embolic complications Stroke Acute Kidney Injury Haematuria Septic arthritis Osteomyelitis Immune mediated vasculitis
- 41. Roth’s Spots
- 42. Janeway Lesions
- 44. Osler’s Nodes
- 45. Clinical signs Fever most common sign(80%) New or changing murmur(48% and 20%) Non specifics viz splenomegaly, splinter haemorrages, petechie, neurol signs, digital clubbing Osler nodes, Roth spots, Janeway lesions Signs of CHF
- 46. Lab Investigations • Blood cultures are key to diagnosis; • Minimum of 3 samples from different sites over 30 min-24 hr; must include anaerobic culture. Positive result is growth of typical microbes in at least 2 samples. • Culture negative samples are caused by prior antibiotic use, fastidious organisms, poor techniques, inadequate blood volume
- 48. Lab Cont’d Echocardiography: Visualising vegetations, Abscesses Structural lesions Ventricular functions CHF diagnosis Predicting embolic complications of IE
- 49. Echocardiography Echocardiography can be: i) TTE ii) TEE TEE more sensitive than TTE in visualising smaller vegetations < 10mm, right sided lesions, PVIE
- 50. Echocardiographic Predictors of systemic embolization: Large valvular vegetations > 10mm in diameter Multiple vegetations Mobile but pedunculated vegetations Noncalcified vegetations Vegetations that are increasing in size Prolapsing vegetations
- 51. Others….. FBC: anaemia, leucocytosis, are common ESR, CRP: usually elevated Decreased C3, C4 and CH50 Pro-calcitonin may be elevated Urinalysis; microscopic haematuria & protienuria E/U/Cr
- 52. Others…… Plasma Glucose to r/o DM Lipid Profile CXR: Septic emboli; features of CHF CT/MRI of the Brain for cerebral complications ECG: 1st degree A- V Block and new IVCD: Bad prognosis
- 53. CXR: Features of CHF Pulmonary infiltrates esp in right sided endocarditis ECG: Conduction defects Myocardial infarction Arrhythmias
- 54. Diagnostic criteria Modified Duke's criteria ( Major & Minor) Major criteria include: Positive blood culture of typical organisms in the absence of a primary focus in 2 or more blood cultures A positive serologic titre for Q fever or PCR for fastidious organisms
- 56. Echo evidence of IE viz Vegetations Abscess Prosthetic valve dehiscence New valve regurgitation
- 57. Diagnostic Criteria • Duke's Minor Criteria: • Predisposing cardiac condition or iv drug use • Fever; Temp > 38 degrees centigrade • Vascular phenomena viz major arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial/conjunctival hhages, Janeway lesions • Immunologic phenomena; AGN, Oslers nodes, Roth spots, positive Rheumatoid Factor
- 58. Microbial evidence: A positive blood culture but not meeting major criteria or a positive serologic evidence of an active infection that can cause IE Echo consistent with IE but not meeting major criteria.
- 59. Guidelines on the prevention, diagnosis, and treatment of infective endocarditis (new version 2009)
- 60. Categories of IE diagnosis Definite IE: Demonstration of microbes in vegetations, on cardiac tissues or on valves Histologic evidence of vegetations on cardiac tissues 2 major Duke’s criteria; 1 major 3 minor or 5 minor criteria
- 61. Possible IE: 1 major and 1 minor; or 3 minor criteria No IE: Resolution of fever under 4 days of antibiotic regimen, absence of microbial and echo evidence of IE
- 62. Goal of Treatment Eradication of causative microbe Treatment of complications
- 63. Treatment Parenteral antibiotics is mainstay of treatment Antibiotics with high MIC/MBC should used Bactericidal antibiotics in combination is a must Antibiotics should be used for 4- 6weeks Antibiotics should be used based on blood culture results
- 64. NVIE with penicillin susceptible organisms( no staph) use iv Pen G 4-6 MU 4 hrly x 4-6 wks or iv ceftriaxone 2g daily x 4 wks plus Iv Getamycin 1mg/kg 8hrly x 2 wks
- 65. For suspected cases of staph endocarditis iv vancomycin 30mg/kg in 2 divided doses x 4- 6wks plus iv gentamycin 1mg/kg 8 hrly x 2 wks
- 66. For Early PVIE and IVDA use vancomycin & gentamycin as above For penicillin allergic patients use vancomycin and gentamycin as above HACEK organisms use ceftriaxone and gentamycin Fungal endocarditis use fluconazole or Amphotericin B
- 67. Indications for surgery viz Failed antibiotic therapy Persistent vegetation after systemic embolization Fungal endocarditis Increase in size of vegetation after antibiotic Rx Valvular damage/destruction
- 68. Complications Cardiac 33-50% Neurologic 25-35% Embolic 15-35% Metastatic < 15%
- 69. Neurologic complications include: Acute encephalopathy Meningitis Embolic stroke Cerebral haemorrhage Brain abscess
- 70. Cardiac Complications CHF Paravalvular abscess Pericarditis Fistulous intracardiac connections
- 71. Embolic complications Stroke Ischaemic extremities Paralysis from embolic infarction of brain or spinal cord Pulmonary emboli Abdominal pain from splenic/renal infarction
- 72. Metastatic Complications Brain abscess Septic arthritis Vertebral osteomyelitis Meningitis Splenic/Renal abscess
- 73. Poor Prognostic Factors • Female Gender • Staph aureus infection • Large vegetation • Aortic valve vegetation • Prosthetic valve • Advanced Age • DM • Immunosuppression • Heart Failure • Acute lung injury • Paravalvalar abscess • Embolic complications
- 74. Prophylaxis • High risk cardiac lesions include Prosthetic valves CHDx viz unrepaired cyanotic heart dx, completely repaired CHDx with prosthetic material/device, repaired CHDx with residual defects Cardiac Transplant recipients with diseased valves
- 75. Procedures requiring antibiotic prophylaxis • Dental procedures • Invasive respiratory procedures • Tonsillectomy • Adenoidectomy • Bronchoscopy with biopsy • Gentiourinary procedures
- 76. Antibiotic prophylaxis Oral amoxicillin 2g 30- 60 mins before procedure i.v ampicillin 2g for those who cannot take orally Oral clindamycin 600mg for penicillin allergic individuals or i.v for those who cannot take orally