Download as DOCX, PPTX
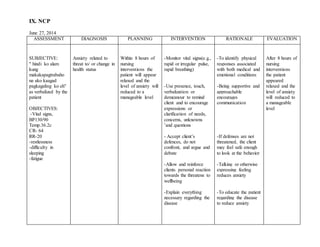
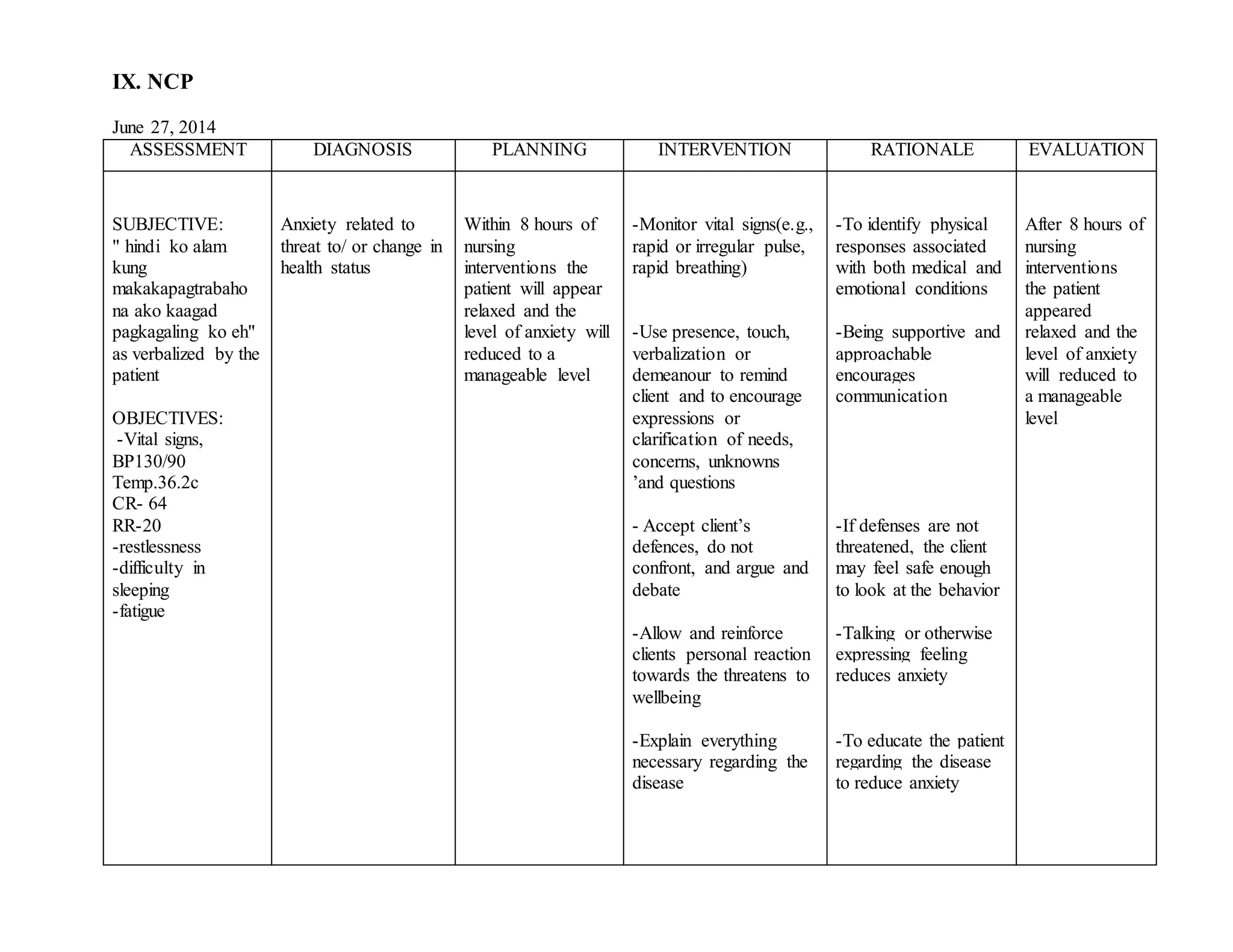
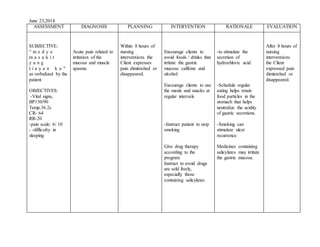
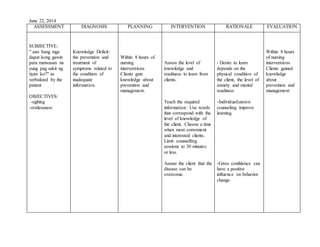
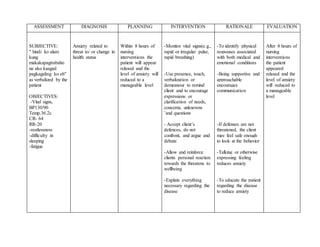
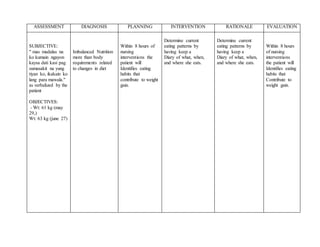

The document contains multiple sections from nursing notes on different patients. It includes assessments of patients' symptoms and concerns, nursing diagnoses, objectives for interventions, details of interventions provided and their rationales, and evaluations of outcomes. Key information includes patients presenting with anxiety about their health, pain, knowledge deficits, and weight gain related to changes in diet. Nurses addressed these issues through monitoring, education, and lifestyle counseling aimed at reducing anxiety and pain levels, increasing knowledge, and identifying unhealthy eating habits within 8 hours of interventions.