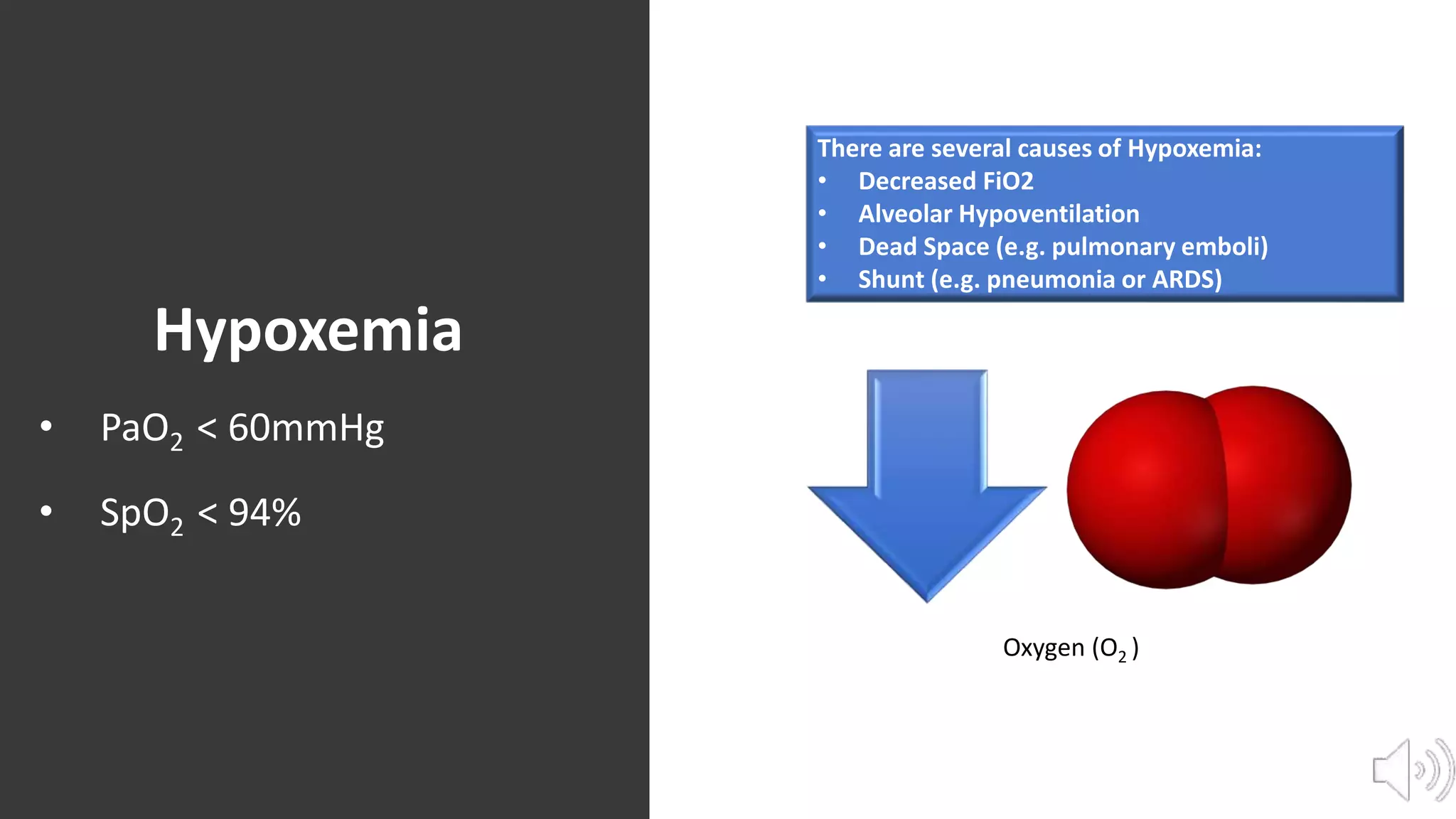
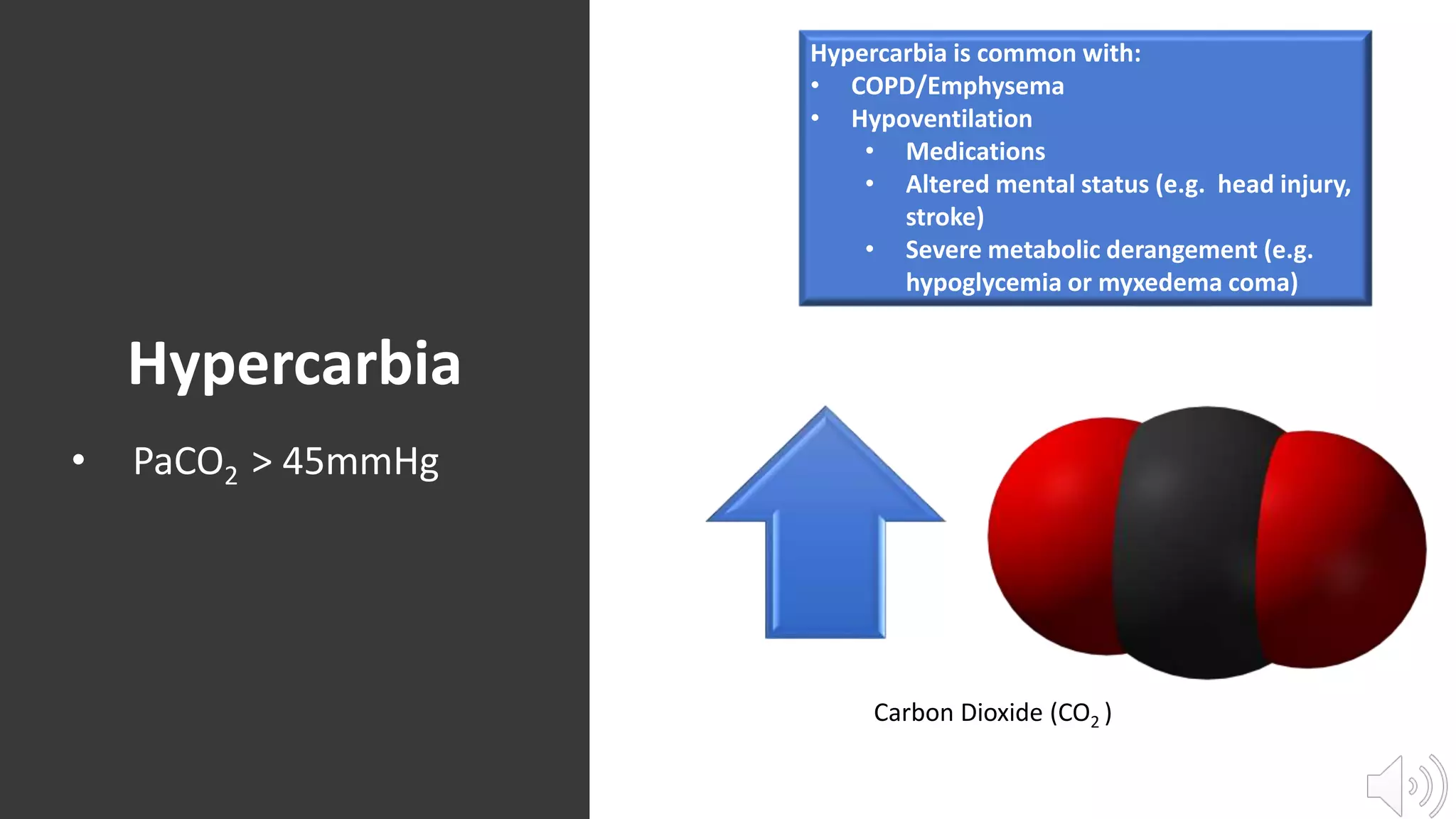
This document outlines the main indications for intubation and mechanical ventilation, including hypoxic respiratory failure, hypercarbic respiratory failure, airway protection, and non-sustainable work of breathing. It defines hypoxemia and hypercarbia, listing common causes and symptoms. Airway protection is needed for those unable to clear secretions due to conditions like stroke, head injury, or medication effects. Intubation is also indicated when a patient's work of breathing becomes too high and non-sustainable to properly oxygenate and ventilate.