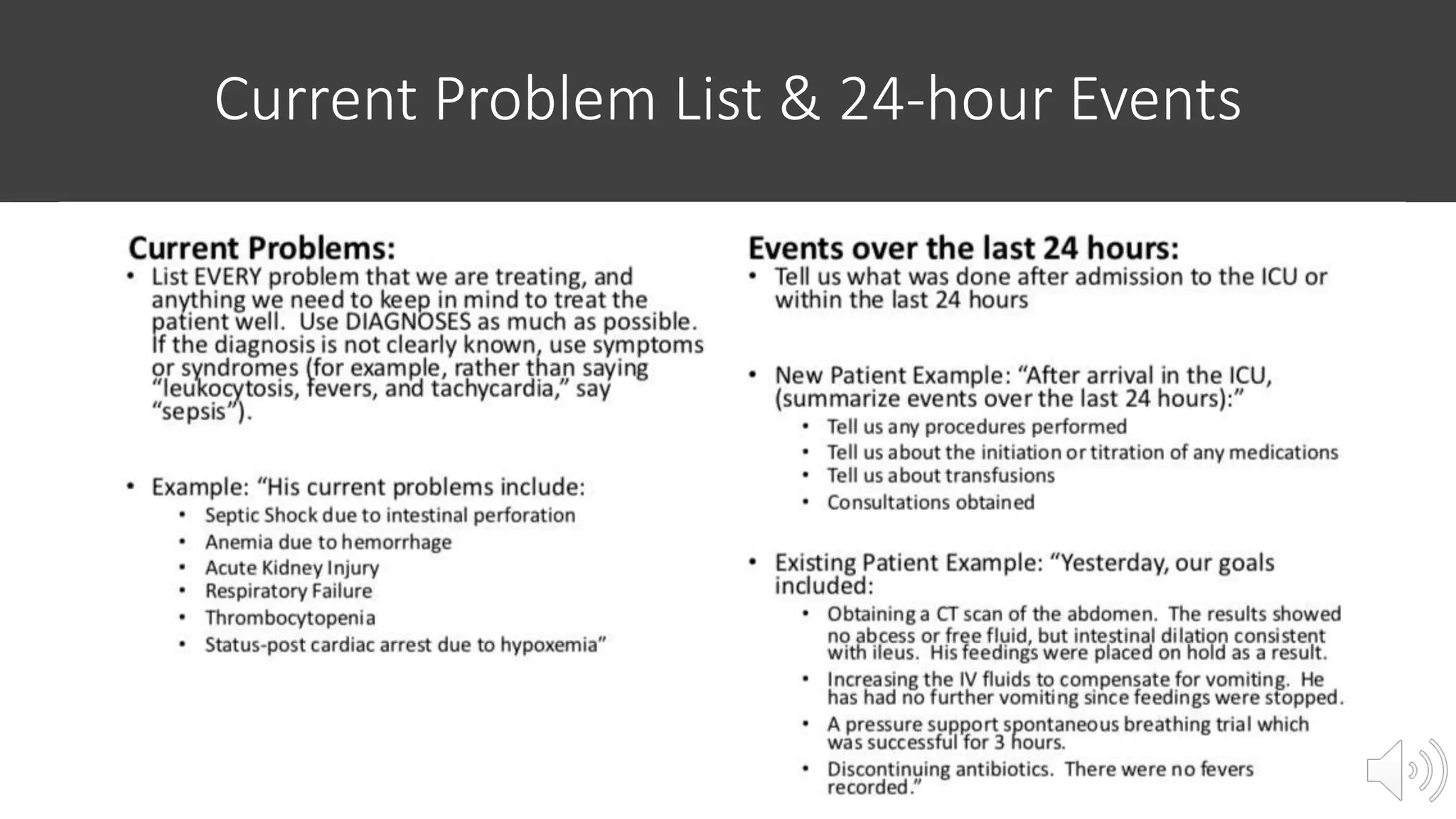
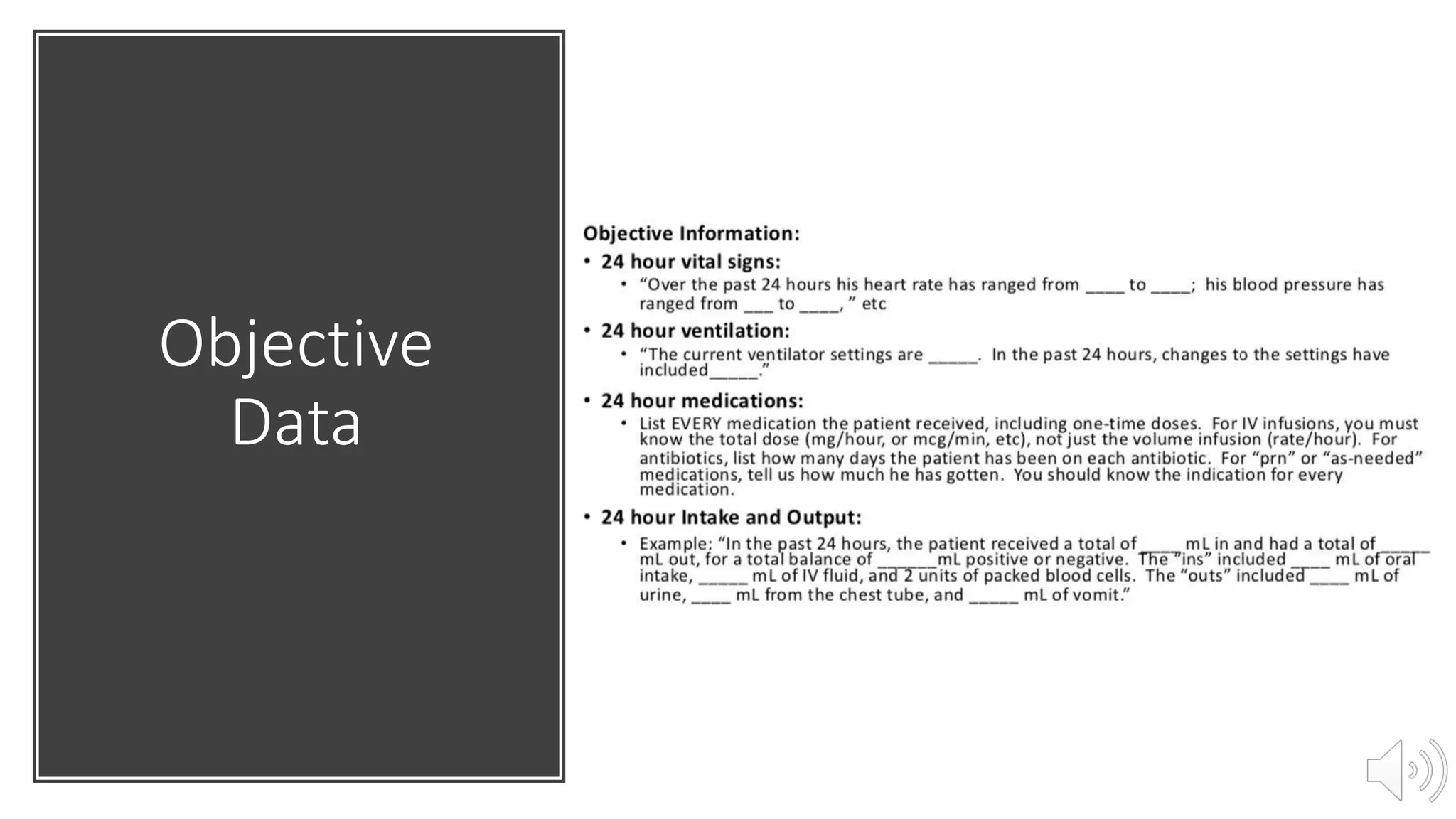
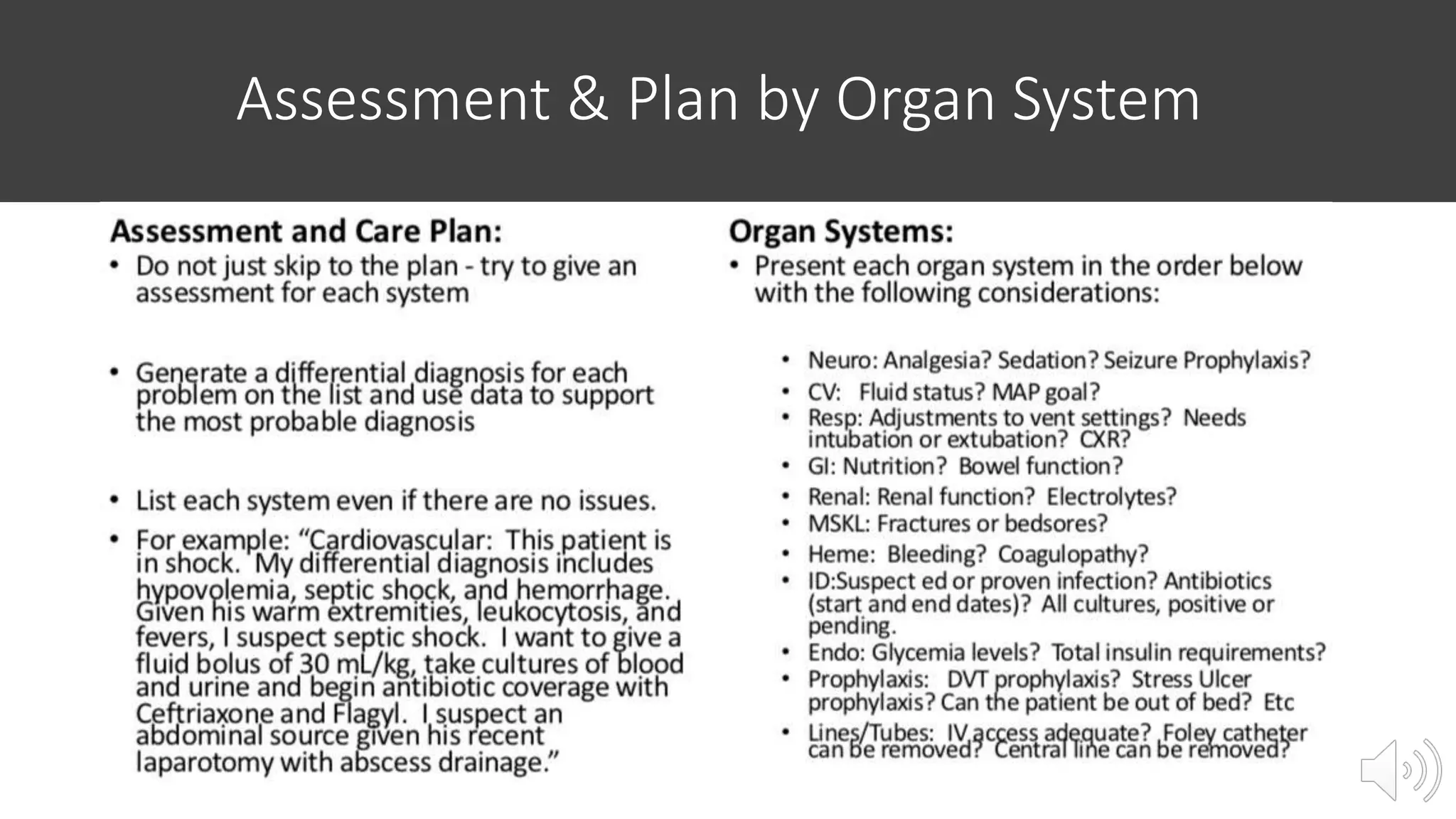
Take ownership of your ICU patients by being organized, involved, efficient and thorough. Use a systems-based presentation template to record and present the patient's past medical history, current problems, procedures, objective data from exams and investigations, and your assessment and plan organized by organ system. This will guide learners in the ICU to effectively present patient information.