Download to read offline
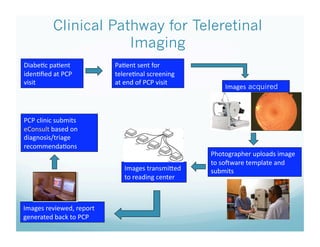
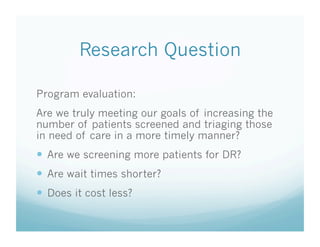
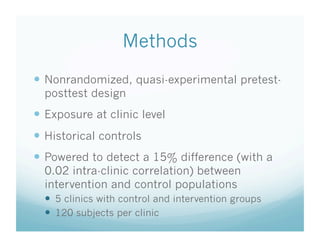
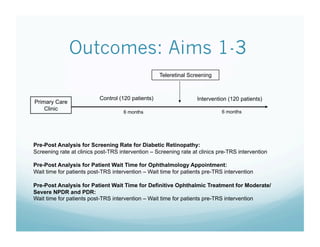
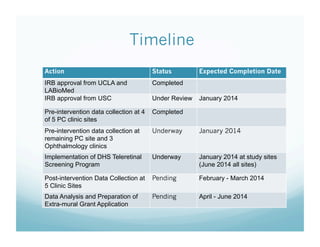


The document outlines the implementation of a primary care-based teleretinal screening protocol in Los Angeles County to address diabetic retinopathy, a significant cause of blindness. It details the project's goals, methods for screening, and aims for evaluation, including increased patient screening and reduced wait times. The initiative involves collaboration between community and academic entities, with ongoing progress reported on approvals, data collection, and the rollout of the teleretinal screening program.


















































![DR PPT[1]2[1].pptx - Read-Only.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drppt121-240211165233-9e17dc66-thumbnail.jpg?width=640&height=640&fit=bounds)

































![How to Craft the "Significance” & "Innovation" [Filler] - 2023](https://cdn.slidesharecdn.com/ss_thumbnails/fillersignificanceinnovation2023-231106193724-1a0824f3-thumbnail.jpg?width=640&height=640&fit=bounds)
