Downloaded 33 times

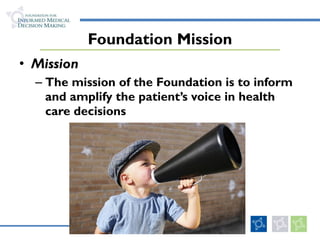
![Practice Policies: Standards, Guidelines and Options Standard: “…at least 95%, perhaps even 99%, of people who are candidates should agree on the desirability of it outcomes Guideline: “…the outcomes must be prefered by an appreciable but not unanimous majority [60% to 95%] of people.” Option: “Outcomes unknown…preferences unknown…preferences indifferent…or preferences split [40% to 60%]” (Eddy DM. JAMA 1990; 263:3077)](https://image.slidesharecdn.com/01-michaelbarry-researchpolicyforum-1-26-11draft-110131130921-phpapp02/85/The-Role-of-the-Patient-s-Voice-in-Improving-the-Quality-of-Health-Care-17-320.jpg)
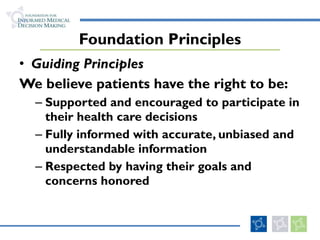
![Shared Decision-Making Model Key characteristics: At least two participants – [clinician] and patient – are involved Both parties share information Both parties take steps to build a consensus about the preferred treatment An agreement is reached on the treatment to implement (Charles C, Soc Sci Med 1997; 44:681)](https://image.slidesharecdn.com/01-michaelbarry-researchpolicyforum-1-26-11draft-110131130921-phpapp02/85/The-Role-of-the-Patient-s-Voice-in-Improving-the-Quality-of-Health-Care-18-320.jpg)

The document discusses the importance of incorporating the patient's voice in health care decisions to improve quality and outcomes. It highlights that patients should be well-informed about their options and involved in discussions regarding their treatments, yet current practices often fall short of this ideal. The foundation advocates for shared decision-making and the use of decision support tools to enhance patient engagement and satisfaction in their health care choices.














































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


