Downloaded 10 times
































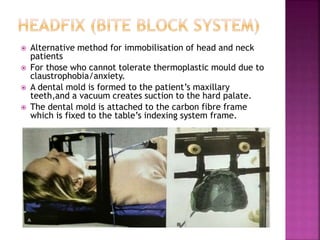
















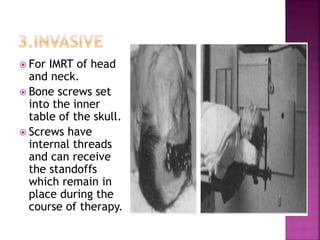






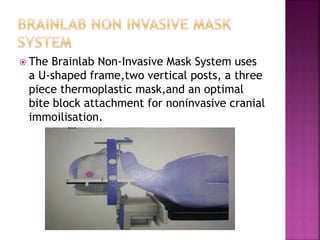



1) Immobilization devices are used to fix patients in a reproducible position for radiation therapy in order to minimize positioning errors and reduce the dose to surrounding healthy tissues. 2) Early immobilization methods included plastic head cups, neck rolls, and plaster casts, while modern techniques use thermoplastic masks, vacuum bags, and foam molds for rigid fixation. 3) Positioning devices like breast boards and knee cradles are also used to maneuver body parts out of the beam path or into a position allowing better beam access for treatment. Precise immobilization combined with IGRT continues to improve the accuracy and safety of radiation therapy.









































































