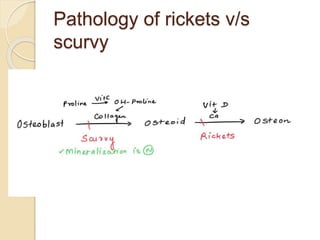
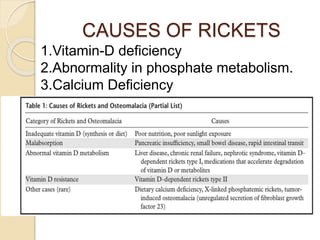
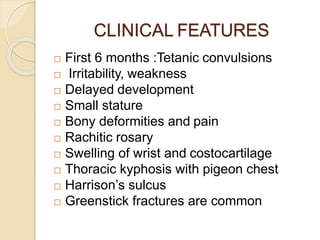
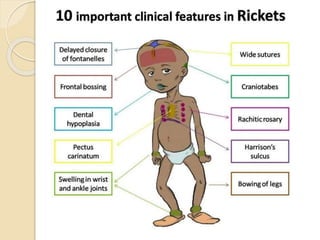
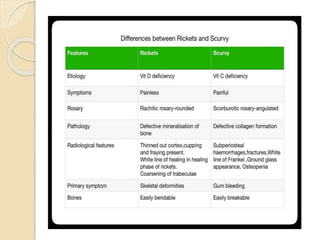
The document discusses the roles of imaging in diagnosing rickets and scurvy, highlighting their pathological features and radiological findings. Rickets is primarily characterized by mineralization failure in the growing skeleton, leading to deformities and specific imaging changes, while scurvy results from vitamin C deficiency, affecting collagen synthesis and causing spontaneous hemorrhage. Both conditions manifest distinct clinical and radiological features that aid in diagnosis and treatment monitoring.






















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








