INTERNSHIP REPORT FORTHE
COURSE MCFTP-001
Submitted to
Indira Gandhi National Open University
in partial fulfilment of the requirement
for the degree of
M.Sc. Counselling and Family Therapy
(MSCCFT)
Name of the Student:
Enrolment No:
Contact Details:
Regional Centre: Delhi 1 (07)
Submitted in
Supervisor: Dr.
7.
75
Weightage ofmarks for external evaluation is 50%. To calculate this, use
the formula given below:
Total marks obtained by the learner ( B )
× 50 = M
1100
Note: The pass percentage for external evaluation is 40%. Therefore if the learner
gets less than 20 marks after calculating 50% weightage, then the student
has to repeat the Internship. In other words, ‘M’ obtained by the student
should be at least 20 to pass.
The external evaluator is required to use the above formula to calculate the
final marks, out of 50, obtained by the learner in external evaluation and to
write this score in figures and in words.
× 50 = .............
1100
(Marks obtained out of 50 in external evaluation to be written in both
figures and words)
..............................................................................................................................
Date: (Signature of External Examiner of IGNOU Panel)
Place:
( B )
(iv)
Internship Report (MCFTP001)
Page| 21
ACKNOWLEDGEMENTS
This internship would not have been possible without the kind support and help of my
supervisor, the psychiatrists and psychologists in IHBAS and fellow interns. I would like to
extend my sincere thanks to all of them.
INTERNSHIP SUPERVISOR
First and foremost, I would like to thank my internship supervisor Her
continuous support and guidance were critical for the successful and timely completion of the
programme in general, and internship in particular.
FACULTY AND STAFF AT IHBAS
Before entering IHBAS I was quite apprehensive if I would be able to fulfil the objectives of
the internship there, would I be allowed to counsel patients and their families, would I even
be allowed to acclimatise by observing sessions when they happen. However, all these
apprehensions were laid to rest soon after joining, as I was encouraged by everyone including
the senior-most faculty and staff repeatedly, to learn and contribute as much as I can.
I am highly indebted to the HOD Psychiatry Prof. Dr. Deepak Kumar, consultant and Asst.
Prof. Dr. Aparna Goyal, chief SRs Dr. Harsha, Dr. Aakanksha Malhotra, Dr. Vaishali
Miglani and Dr. Seshan Varshney, and other SRs and JRs of Unit 2 including Dr. Adhil K. for
their valuable support during the internship in their esteemed organisation.
I would like to especially thank Dr. Mohd. Nahid Irshad for making me feel comfortable,
encouraging me to get involved in cases even before I had become acclimatised, and
spending a lot of time discussing and problem-solving with me about the very specific
nuances of cases and generally, being supportive. The time that we spent together exploring
various cognitive phenomena in the patients as part of their assessment and diagnoses was
probably one of the best parts of the internship for me. This period gave me the confidence
and set the tone for the internship, that led me to boldly comment, suggest and question –
leading to a significant outperformance of any expectations that I had from the internship.
14.
Internship Report (MCFTP001)
Page| 22
I’m also thankful to the Associate Professors Dr. Amit Khanna, Dr. Shipra Singh, Dr.
Pratibha and Dr. Shahzadi Malhotra, Asst. Professor Dr. PHiteshn B. Yannawar, and Ms.
Sampa Sinha for answering all the questions that I bothered them with, and taking my inputs
and suggestions during sessions and discussions in a positive and encouraging way.
While at IHBAS I was treated as a fellow Mental Health Professional and given the
opportunity to participate in patient care and all activities which are normally open for the
psychiatry and psychology students of IHBAS. I was involved in active patient-care, allowed
to attend case conferences, movie-cons, knowledge sharing sessions and attend the grand-
rounds where the seniormost psychiatrists, clinical psychologists, counsellors and Psychiatric
Social Workers shared their perspectives and provided guidance.
I was allowed access to almost all parts of the hospital, made a part of the ward-rounds and
even assigned specific responsibilities pertaining to the cases, as will be obvious from the
quality of this report.
All these contributed to making this an unmatched learning experience.
FACULTY AT IHE
I would like to express my gratitude towards , Coordinator of the IHE Study
Centre and former Asst. Coordinator for providing their permission and a
reference letter at a very short notice which allowed me to apply for internship in such an
esteemed organisation.
I’m also thankful to , Asst. Coordinator of the IHE Study Centre for her
continuous and prompt support on all matters and the academic counsellors
for encouraging experience-based case discussions during the theory
sessions which also contribute immensely to the students’ learning.
15.
Internship Report (MCFTP001)
Page| 23
TABLE OF CONTENTS
Annexure A: Certificate of Assigning an Approved Guide for Internship................................3
Annexure B: Evaluation Sheet...................................................................................................5
Annexure C: Certificate of Completion of Internship .............................................................15
Annexure D: Certificate of Authenticity..................................................................................17
Permission for Submitting Typed Internship Report...............................................................19
Permission for Submitting Spiral Bound Report .....................................................................20
Acknowledgementss ................................................................................................................21
Table of Contents.....................................................................................................................23
List of Figures..........................................................................................................................26
Chapter I: Introduction.............................................................................................................29
1. Introduction to the Internship...........................................................................................29
2. Organisation Profile.........................................................................................................30
3. Internship at Clinical Mental Health Unit, IHBAS..........................................................31
4. Internship Report .............................................................................................................32
Chapter II: Record of Acclimatisation Sessions......................................................................35
Acclimatisation Report ........................................................................................................35
Field Notes/Session Transcripts...........................................................................................55
Supervisor’s Comment Form...............................................................................................71
Chapter III: Record of Counselling Case Work 1....................................................................73
Referral & Intake .................................................................................................................73
Intervention Adopted ...........................................................................................................77
Termination & Follow-Up...................................................................................................84
16.
Internship Report (MCFTP001)
Page| 24
Difficult Situations Encountered..........................................................................................86
Barriers in Communication and Handling Emotional Outbursts.........................................86
Reflections ...........................................................................................................................87
Permission/Consent Letter...................................................................................................89
Tools: Case History and Mental Status Examination ..........................................................91
Field Notes/Session Transcripts.........................................................................................111
Supervisor’s Comment Form.............................................................................................123
Chapter IV: Record of Counselling Case Work 2 .................................................................125
Referral & Intake ...............................................................................................................125
Intervention Adopted .........................................................................................................129
Termination & Follow-Up.................................................................................................140
Difficult Situations Encountered........................................................................................143
Barriers in Communication and Handling Emotional Outbursts.......................................143
Reflections .........................................................................................................................143
Permission/Consent Letter.................................................................................................145
Tools: Case History, Mental Status Examination & IPDE................................................147
Field Notes/Session Transcripts.........................................................................................165
Supervisor’s Comment Form.............................................................................................179
Chapter V: Record of Family Therapy Case Work 3 ............................................................181
Referral & Intake ...............................................................................................................181
Intervention Adopted .........................................................................................................185
Termination & Follow-Up.................................................................................................201
Difficult situations encountered.........................................................................................202
Barriers in Communication and Handling Emotional Outbursts.......................................203
Reflections .........................................................................................................................203
17.
Internship Report (MCFTP001)
Page| 25
Permission/Consent Letter.................................................................................................205
Tools: Case History, Mental Status Examination & Family Interview .............................207
Field Notes/Session Transcripts.........................................................................................233
Supervisor’s Comment Form.............................................................................................247
Chapter VI: Record of Family Therapy Case Work 4 ...........................................................249
Referral & Intake ...............................................................................................................249
Intervention Adopted .........................................................................................................254
Termination & Follow-Up.................................................................................................268
Difficult situations encountered.........................................................................................271
Barriers in Communication and Handling Emotional Outbursts.......................................271
Reflections .........................................................................................................................272
Permission/Consent Letter.................................................................................................273
Tools: Case History and Mental Status Examination ........................................................275
Field Notes/Session Transcripts.........................................................................................303
Supervisor’s Comment Form.............................................................................................319
Chapter VII: References .......................................................................................................321
Appendices.............................................................................................................................323
Appendix 1: Reference Letter from IHE ...........................................................................325
Appendix 2: Application Submitted to IHBAS .................................................................327
Appendix 3: Certificate of Completion of Internship at IHBAS .......................................329
Appendix 4: IHBAS Circular and Log Sheet ....................................................................331
Appendix 5: Basic Genogram Symbols.............................................................................337
Internship Report (MCFTP001)
Page| 29
CHAPTER I: INTRODUCTION
1. INTRODUCTION TO THE INTERNSHIP
As a counsellor and family therapist, one would be helping individuals in different stages of
the human life span and family life cycle, each having a general problem with unique
specifications to the self and the family.
MCFTP-001 ‘Internship’ involves original, rigorous counselling and family therapy work
carried out with substantial independence by each M. Sc. student of the Counselling and
Family Therapy Programme. The course involves carrying out the Internship work for the
required duration in a requisite setting to learn practical application of the theoretical
knowledge. It enables the Interns to integrate and apply counselling and family therapy
knowledge and intervention to promote optimum health of individuals or groups.
It is designed to give the students hands on experience in counselling and family therapy. The
internship intends to help students:
- Achieve knowledge and skills, as well as develop competencies for entry-level
practice in various specialization areas of counselling and family therapy.
- Demonstrate expertise and the mastery of knowledge of current practices and
theoretical frameworks of counselling and family therapy.
- Acquire hands-on experience in personally conducting counselling and family therapy
sessions in a range of situations
- Understand the practical aspects of conducting counselling and family therapy
sessions
- Learn the application of theoretical concepts and approaches of counselling and
family therapy in real life situations
- Gain an enriching and comprehensive insight into the recent concepts, current
knowledge regarding the management of diverse disorders, complex family situations
and personalities, and problems encountered in effective counselling and family
therapy; and
22.
Internship Report (MCFTP001)
Page| 30
- With opportunities for developing competencies and prepare them to conduct
counselling and family therapy by providing practical training in the field of:
o child and adolescent counselling and family therapy
o marital and family therapy and counselling
o substance abuse counselling and family therapy
o geriatric counselling and family therapy
o crisis and trauma counselling and family therapy
o gender and sexual abuse counselling and family therapy
o HIV/AIDS counselling and family therapy
o Counselling and family therapy in chronic physical illness; etc.
The entire internship was conducted as per the instructions given in the Internship Manual for
MCFTP001 (Chadha & Ratra, 2011). The information in this section is also based on it and
the rest of this report also follows the suggestions given in the manual.
2. ORGANISATION PROFILE
The Institute of Human Behaviour and Allied Sciences (IHBAS), formerly known as Hospital
for Mental Diseases, Shahdara, is a mental health and neurosciences research institute based
in Shahdara, New Delhi, India. IHBAS is one of the largest mental hospitals in the world in
terms of number of patients served and area of campus. (Summary Highlights of Annual
Report 2016-17, 2017) It also houses the state mental health authority (SMHA) of Delhi.
IHBAS was established in 1993, in response to a Supreme Court verdict, transforming
previous HMD into a centre for treatment, training, and research (Kukreti & Jiloha, 2018). It
is an Autonomous Society under administration by the Delhi Government. It has three
clinical and all other para and allied branches.
The vision of IHBAS is to be one of the leaders in the country and in the world for promoting
mental health, neurosciences, behavioural and allied sciences through multidisciplinary
patient care in partnership with communities, developing future group of professionals and
paraprofessional leaders through formal and semiformal training programmes and expanding
scientific knowledge and its application through front-line research. (Vision, 2024)
23.
Internship Report (MCFTP001)
Page| 31
The mission of IHBAS is to advance the mental and neurological health of populations by
practicing evidence based multidisciplinary scientific health care approaches that are novel,
adaptive, and ethical, conduct research of high standard and develop human resource in these
fields. The institute adheres to quality assurance, integrating into practice the prevailing
norms for human rights and diverse value systems of persons and populations while
accomplishing this mission. (Mission, 2024)
The Aims & Objectives of the institute are:
- To provide high quality super specialty health care using state-of-art technology in
Mental health, Neurosciences, Behavioural and Allied sciences.
- To conduct research of high standard in the field of Mental health, Neurosciences and
Behavioural sciences.
- To provide comprehensive training for MD, DM, M. Phil. & PhD courses in the field
of Mental health, Neurosciences and Behavioural sciences and research activities on
current interest.
Various cost-effective measures have been taken to improve services. Quality of patient care
has improved remarkably. Duration of stay of patients has been reduced. Good quality
essential drugs are provided to the patients free of cost by the institute. (Aims & Objectives
Of IHBAS, 2024)
Considering the internship at IHBAS fulfils the requirements specified in the MCFTP001
Internship manual - the criteria set by the University, I chose to do my internship at this
organization.
3. INTERNSHIP AT CLINICAL MENTAL HEALTH UNIT, IHBAS
This internship was carried out for a period of more than 300 hours over a course of 64 days
with a short 4-day break in the middle mandated by G20 related restrictions.
The internship helped me to get hands on experience in the areas of Counselling, Family
Therapy and Clinical Psychology. I was given the chance to assess clients and learn the
planning of strategies to help clients from different settings to overcome their problems.
24.
Internship Report (MCFTP001)
Page| 32
I was assigned to Unit 2 where I was posted initially in Female B Ward (FBW) which is the
semi-closed ward for female patients and then in the Children and Adolescents Psychiatric
Wards (CAPW) both Male and Female which are the semi-closed wards for children and
adolescents. The Mother Child Unit (MCU) and Adolescent Deaddiction Unit (ADU) are also
co-located with CAPW and managed by the same team of psychiatrists, clinical psychologists
and counsellors so I also got the chance to interact with the patients admitted there and their
families.
I was also required to attend OPD (Out Patient Department) on Tuesday and Friday, the
designated days for Unit 2 OPDs. In addition, I also visited the Emergency SOF (Short
Observation Facility), Person Isolation Facility (PIF) and Private Wards to interact with
patients and their families.
Apart from this I was also allowed to visit Female Open Wards (FOW), Male Open Wards
(MOW), semi-closed Male Wards (MAW/MBW), Female A Ward (FAW), Drug Abuse
Treatment and Rehabilitation Centre (DATRC), Dual Diagnosis Unit (DDU) and
Occupational Therapy (OT) department.
Due to the independence, encouragement and the intense exposure, in such a short timeframe
I learnt to deal with diverse populations including children, adolescents and adults.
Especially, helping and managing families. I also learnt to conduct various assessments and
interviews and properly interpret the results to develop a plan to counsel the clients.
Activities carried out during the internship include assessment and diagnosis, including
interviewing, case history taking, administration of tests, scoring and interpretation of the test
results and arriving at correct diagnosis of the problem, and finally, counselling for both
individuals and families.
4. INTERNSHIP REPORT
As advised in the internship manual, this Internship Report has been prepared by compiling
the written records of the acclimatisation sessions and of the four case-works. The duly filled
in requisite annexures and enclosures have also been included.
This report covers a selection of four such cases - including details of the sessions,
psychological testing and interventions carried out. Of the four records, two case records are
25.
Internship Report (MCFTP001)
Page| 33
of individual counselling involving 8+ sessions and two case records are of family therapy
involving 13+ sessions.
The internship manual advises that the cases selected for presentation in this report should
belong to at least three different areas from the given list. Accordingly, I have included all
cases pertaining to different areas from the list.
In this report, the name of the client, and other sensitive information that could help identify
the client, has been replaced with a dummy placeholder for confidentiality reasons in line
with the guidelines in sec. 4.06 and 4.07 of the Ethical Principles of Psychologists and Code
of Conduct (American Psychological Association, 2010). Section 4.06 states that:
“…psychologists do not disclose confidential information that reasonably could lead to the
identification of a client/patient, research participant, or other person or organization with
whom they have a confidential relationship unless they have obtained the prior consent of the
person or organization or the disclosure cannot be avoided…”
Section 4.07 states that:
“Psychologists do not disclose in their writings, lectures, or other public media, confidential,
personally identifiable information concerning their clients/patients, students, research
participants, organizational clients, or other recipi- ents of their services that they obtained
during the course of their work, unless (1) they take reasonable steps to disguise the person
or organization, (2) the person or organization has consented in writing, or (3) there is legal
authorization for doing so.”
In addition, in place of my usual preference of using the term ‘client’, ‘family member’ etc.
this report makes use of the terminology as used in the hospital setting - patient, attendant etc.
considering that’s where these cases were worked upon.
To summarize, the internship report has been prepared according to the instructions given in
the manual, while also keeping ethical considerations in mind.
26.
Internship Report (MCFTP001)
Page| 35
CHAPTER II: RECORD OF ACCLIMATISATION SESSIONS
ACCLIMATISATION REPORT
INTRODUCTION
At the beginning of the internship, the first task was to get acclimatised to the surroundings
by observing sessions and interacting with patients and their families under supervision.
Acclimatization involves the gradual adaptation and familiarization with the unique
dynamics, challenges, and nuances within therapeutic settings. It is important to learn to
handle ethical dilemmas, establish rapport with clients, and integrate evidence-based
practices.
Acclimatization ensures that professionals develop sensitivity, resilience, and competence in
addressing diverse client needs while learning from the experts who are already doing it.
Ultimately, this process would enhance their effectiveness in providing client-centred care
and create a supportive therapeutic environment.
As advised in the practicum manual for MCFTE04, acclimatisation happened as I observed
the seniors while they were engaged in counselling and treating patients and their families. In
addition, they observed me while I interacted with patients under their supervision, and gave
me suggestions and feedback to improve. During the initial days, this was my focus.
I wanted to make sure that I understand the patients, their families, issues and concerns of the
patients and their families, the place and its functioning and my role in that place before I got
involved with patient and family care. As an outsider to the setup, I didn’t want to cross any
expected lines, so I was extra careful in the first two weeks.
Fortunately, everyone I interacted with at the hospital was very supportive. This helped in
significantly accelerating the process of acclimatisation. And, within 10 days or so I started
feeling like I wasn’t an outsider but a part of the team, and it was my own workplace. The
people there felt like colleagues and they treated me as such, even the most senior ones.
27.
Internship Report (MCFTP001)
Page| 36
SESSION DETAILS
In the first week itself very many client sessions happened that gave me the opportunity to
acclimatise. As suggested, out of these I’m reproducing four of the sessions below. The
discussions for this activity conducted during the sessions are detailed below along with
observations and comments.
Please Note: These sessions are not listed according to the date, but according to their order
in the counselling and therapy process.
Session 1
- Aim: Intake of the patient
- Date and Duration: ; 1 hour
- Participants: Kala (Patient) and Hitesh (Husband/Attendant)
- Emotional Atmosphere: Noisy
- Seating:
Figure 1: Acclimatization Session 1 - Seating Arrangement
The patient had been admitted by her husband in the emergency. She was currently in the
Short Observation Facility (SOF) and the goal was to understand the issues and
diagnose/validate diagnosis.
The patient and her husband were called to the interview desk placed in the SOF The
husband informed that Kala was born in Almora. They have their own howe and family
income is about Rs. 10,000 per month. They have been married for 22 years. She was
educated till 8th
as her father didn’t want to educate her. He does a job in a private company.
28.
Internship Report (MCFTP001)
Page| 37
After this information was gathered, based on which the following genogram was drawn.
Figure 2: Acclimatization Session 1 - Genogram of Kala's Family
After this the interaction continued. The interaction was in Hindi, it has been translated and
reproduced below in English.
T: Since when does she have the problem?
A: This started 1.5 years back. She took medicine for 8-9 months, till then everything was
fine. Then there was a problem, my father expired – because of which she had to leave the
medicine – because she became sedated after taking medicine. Then we felt she became okay,
so we left the medicine.
T: What are the symptoms currently?
A: Talks too much. Breaks things – whatever she sees, she picks and throws. Hitting hands
and legs. Accusing.
T: Accusing people? [Clarification question]
A: Accusing me. That I watch my sister a lot and I give her money. There was a bachelor
living on rent – she used to favour him a lot. Our daughter is young so I asked him to vacate –
she now asks me why I did so.
29.
Internship Report (MCFTP001)
Page| 38
T: Does she see/hear something that others can’t?
A: No. But she was calling the doctor Chacha ji.
T: What happened to her in the first episode?
A: Excessively waving hands and legs. Getting angry without reason. Gesturing in the air.
Her mouth keeps moving by itself. She was sedated. We had to bathe her. She used to do
pray all day.
T: What about the current episode?
A: It’s been going on for 3 days. She touches everyone’s feet, and asks to touch. She takes
water – or anything else – and sprinkles on us.
T: And, between the episodes?
A: She was unable to sleep. She used to get up and sit.
Then the husband started sharing other concerns.
A: Kala puts phone in her ears and keeps talking to her mother who keeps giving her stress.
“You should lock the home” and “Keep your children separate”, and what not! She even calls
the right thing wrong for about 2- 2.5 years. I have been living away since June due to work.
T: What else?
A: She has panic – palpitations (once in 1.5-2 weeks) and also has anxiety. She used to sleep.
Her mother does not trust me as much now.
T: Does she say big things about herself? [Megalomaniac thoughts]
A: “I am Laxmi. Touch my feet.”
T: Any religious behaviours?
A: She prays. Much more during illness.
While this conversation was going on the patient bent and swung her hand.
30.
Internship Report (MCFTP001)
Page| 39
T: [looking at the patient] What are you trying to catch?
P: Parrot.
T: Is it day or night?
P: Day.
[T looks at A who wanted to say something, and indicates him to talk.]
A: Even my daughter has told me you’re not my father now. Kala says her father has passed
away. Her daughter has passed away. She tells our son to marry our daughter.
While the symptoms of the patient were observable, as the husband was living away for the
past few months, he had limited idea about the current set of symptoms.
A session was conducted with the son immediately afterwards – again limited information
was obtained. However, he did mention that there was a fight at home 3-4 days back, after
which the patient became silent and began ruminating.
The son informed that the patient lived in the daughter’s room and spent most time with her.
There was limited interaction with other family members So, it was then decided to interview
the daughter to add more details to the case history. However, the daughter was not in Delhi
at the time.
It was decided by the psychiatrists to admit the patient and start pharmacological treatment
as the diagnoses was clear. That being the case, I did not have further involvement in this
case as there was limited scope of counselling or therapy while the patient was so severely
symptomatic. The family did not seem to be in immediate need of counselling though a
psychoeducation session would have helped.
The symptoms had not receded when I was shifted to the other ward, so I did not get a chance
to interact with the daughter or the other family members in follow up sessions.
31.
Internship Report (MCFTP001)
Page| 40
Session 2
- Aim: Detailed work-up including MSE.
- Date and Duration: ; 1 hour
- Participants: Sana (Patient) and Sabina (Mother/Attendant)
- Emotional Atmosphere: Loud
- Seating:
Figure 3: Acclimatization Session 2 - Seating Arrangement
The patient had been admitted by her mother and elder brother earlier. In this session, the
objective was to do a detailed work-up including MSE to understand the case better.
The patient was brought to the room by her mother. The psychiatrist took a conversational
style and asked questions from the Case History Format and MSE but not necessarily in any
set order. The session happened in Hindi. The key points were noted and have been presented
below after translation to English.
The mother reported that symptoms have been prevalent since 2014/15 after Sana’s elder
brother, who she was very close to, was murdered in 2013. She was first admitted in 2015.
While giving her developmental history, the mother mentioned that she had attempted to
abort when she was pregnant with the patient, but the attempt was unsuccessful. The patient
was born very late at 10.5 months with a weight of 5 kg. The delivery was normal and there
were no other issues during or after the delivery.
Apart from this the mother reported that she has redness on her head, where they apply
garlic paste. The doctor did not deem this important for further probing.
32.
Internship Report (MCFTP001)
Page| 41
After this information was obtained from the mother for the genogram (reproduced below).
The only noteworthy new information that emerged was that Sana’s father has alcohol
dependency issue and his elder brother has drug addiction issues.
Figure 4: Acclimatization Session 2 - Genogram of Sana's Family
Observation: While the above conversation was going on, Sana stands up and beats the table
saying random words. She did not respond to the psychiatrist.
T: Has she increased her religious rituals since the illness has started? [Over-Religiosity]
A: Earlier she was more regular. Now the frequency has decreased.
T: Does she have episodes of normality?
A: Yes. Only drowsiness due to medicines is there.
T: Does she always behave like this in her illness?
A: Yes. Though earlier she used to hear voices – of cat crying. [Auditory Hallucinations]
T: Does she take drugs or alcohol?
A: No
Then without any prompting the attendant said that Sana starts crying about her brother.
T: Any problems during the lockdown?
33.
Internship Report (MCFTP001)
Page| 42
A: She used to bathe a lot – while wearing clothes. She used to take-off clothes in front of
anyone. She used to hit – both herself and us. She used to run away from home – very far
away. She used to lie down on the floor, on the footpath.
T: Any megalomaniac thoughts?
A: Yeah. I’m going to marry and go to Mumbai.
T: Asked for new things?
A: Yes. During periods she gets worse.
Once again, she adds information irrelevant to the question, indicating she might have a need
to express herself – and talk to someone regarding the child’s illness or she’s tense about it.
T: When did the current episode start?
A: 4-5 days back. She was also admitted in emergency about 45 days back. She accuses us –
that we don’t give her food and clothes. She considers her younger brother to be enemy, even
her elder sister. Only likes uncle’s wife and children. Loves her elder brother and father. She
abuses. Stubbornly demands food, money and clothes. We have to take medicine from
outside.
T: [looking at P, MSE questions] Is it day or night?
P: There’s light.
T: Who is with you?
P: Asif (younger brother) [Wrong answer, not present]
T: Where do you live?
P: Phone.
A: She salutes everyone. Sings songs. Dances. Talks to herself when alone. Gestures with
fingers. Counts on the inch-tape [used in tailoring]. Gets agitated by her brother and sister.
34.
Internship Report (MCFTP001)
Page| 43
She’s demanding like a young child – “get clothes stitched for me”. When she’s ill, she
hoards garbage. [Again, the mother speaks without question.]
T: Is she able to urinate/defecate normally?
A: She did it in her clothes earlier.
P: [loud and irrelevant] Talk softly.
T: When was her last period?
P: [loud and irrelevant] It’s my papa.
A: 5 days back. On time. For 5-6 days. Normal. She always becomes ill during periods. She’s
very scared of insects since she’s gotten ill. Cats and dogs too. She says “look something’s
walking on my hands and head” [Tactile Hallucinations]
P: [loud and irrelevant] Papa. [Pause] Sunday. Monday.
This session was wrapped up after collecting some more information. Later a session with the
brother was held, where no new facts were revealed.
There were doubts about this being a case of MR, however, considering the current symptoms
it wasn’t possible for an intelligence test to be conducted. Her past report cards were called
for – which showed average performance. VSMS conducted in 2017 was used to ‘diagnose’
moderate MR, however, that is inappropriate use of the test so a proper IQ assessment was
planned after patient gets better – also, it would enable them to get a disability certificate
made.
I had some sessions with the family to counsel them – especially, psychoeducation and
management of the patient. When my internship got over, she was still admitted, undergoing
pharmacological treatment.
35.
Internship Report (MCFTP001)
Page| 44
Session 3
- Aim: Psychoeducation
- Date and Duration: ; 1 hour
- Participants: Anil (Brother/Attendant)
- Emotional Atmosphere: Tense
- Seating:
Figure 5: Acclimatization Session 3 - Seating Arrangement
Rani was admitted to the hospital before I joined. She was diagnosed as F20.0 Paranoid
Schizophrenia as per ICD 10 (World Health Organisation, 1993) after detailed work-up
(Case History and MSE) were done.
She’s a 38-year-old unmarried female living with her father and brother.
She was admitted to the hospital by her brother. She was brought in a dishevelled state – her
hair was completely matted – almost like a bird’s nest. She was not allowing to cut off the
hair and had to be counselled, after which she relented and the hair were chopped off by the
barber.
She had reported tactile hallucinations – “Ants are crawling all over.” She was sent for a
derma referral, but it was found to be psychosomatic in nature. She also complained of
‘leeches’ everywhere, including in the food and water.
She also had ‘delusions of persecution’ against her brother, who she felt was trying to harm
her and her father, and used to beat them. She expressed her desire to be discharged and go
back home and take care of her father.
36.
Internship Report (MCFTP001)
Page| 45
Based on the observations of the ward staff and during sessions, the father was suspected to
have substance dependence and might possibly have an undiagnosed psychological
condition. The genogram of the patient’s family is given below. The brother is engaged and
supposed to get married soon.
Figure 6: Acclimatization Session 3 - Genogram of Rani's Family
He reported that he was trying to get her married – even to his own friend, so that she could
settle in life. However, she developed this illness. According to him, she had some issues even
before Covid. But, during Covid she stayed locked in single room, so her situation
deteriorated significantly.
Since then, the issues became more and more complex. Gradually, grooming completely
stopped. And, she started calling the police. That is when she was brought to the hospital.
The attendant had been called for a session to get an update on the health condition, but it
turned into a psychoeducation session.
A: Sir, what has happened to Rani? [Looked anxious and flustered]
T: You look anxious Anil. What happened?
A: She keeps saying such bad things. Now, she's saying I murdered my mother for insurance,
and I tried to kill her. She used to say that I hit her and my dad. But now it’s going to the next
level. Why is she lying like this?
37.
Internship Report (MCFTP001)
Page| 46
T: Relax Anil. Have a glass of water. [He was offered a glass of water which he drank.]
After he calmed down.
T: Are you better now?
A: Yes sir. Please tell me why this is happening.
T: It is because of her illness. This is how the patients of this illness often do. What do you
know about her illness?
A: Madam told me she has schizophrenia... Isn't that the same thing in that English movie...
About the mathematician.
T: Which movie? A Beautiful Mind?
A: Yes.
T: Correct, that’s it. What do you know about schizophrenia?
A: That people see things and hear things... That's why we brought her here. She thinks there
are ants roaming about all over her body. And she used to talk to herself. And then she started
fighting with everyone. She says I beat her. She even called the police. We did not have any
option – we had to bring her here. It was too difficult for us! Even we did not want to admit
her to a mental hospital [sense of Stigma], however, we were not left with a choice.
T: Yes. What you’re saying makes sense. And all the things that you have mentioned – they
are normal in her illness.
A: So, all the patients of this illness call the police?
T: Not all. But she has paranoid schizophrenia. And, it isn’t unusual for patients of paranoid
schizophrenia to be scared and take actions to protect themselves – like calling the police.
The counsellor explained in detail, sharing some more examples and working on allaying his
anxieties. The to and fro continued as Anil asked more questions related to the illness.
T: So now, do you have any more questions about it?
38.
Internship Report (MCFTP001)
Page| 47
A: No. I'm feeling alright now. I was very worried in the morning - why is this happening.
Now I understand...
T: Good.
A: But, why does this happen? Will her children also have the problem? What should I tell
my friend, if he asks.
T: That’s an important question…
The counsellor explained the aetiology. Upon learning about the high possibility of genetic
disposition in his family, there was again some to and fro about whether his children also
might be impacted because of it. Then it drifted to another topic…
A: So, will she ever be fully treated? Fully cured? Or will it go on like this only?
The counsellor explained the prognosis and the importance of proper and continued
treatment. After this the conversation moved towards treatment and management of the
patient. The prognosis and treatment were explained. The role of the family members and
what they could do to help in the situation was also explained.
A: Sir, I’m not sure what to do. What should I do about her? Should I ask my friend to marry
her or not? If she doesn’t get married, it will be too difficult for me… I’m a middle-class
person – not very rich. That is why I had to come to a govt. hospital.
The counsellor counselled him further on some of these dimensions, and suggested him to
have an open and honest discussion with his friend about the situation and let him decide –
whether he likes Rani enough to marry her, in spite of her medical situation is his choice.
Nobody can, and nobody should, decide on his behalf.
With this the session proceeded to conclusion.
A: Thank you, sir! Today a lot of my doubts were cleared. I was so worried when I came –
but I am feeling a lot better now. Can I meet you again if I have any questions?
T: Of course, Anil!
With this the session was concluded. A few days later the patient was discharged with
instructions to continue treatment in OPD or a hospital near her home. Two weeks later, the
patient was seen in the OPD from a distance – she seemed to be calm and stable.
39.
Internship Report (MCFTP001)
Page| 48
Session 4
- Aim: Pre-Discharge Counselling (focused on treatment compliance and exploring IPR
issues contributing to illness)
- Date and Duration: ; 1 hour
- Participants: Huma (Patient), Saif and (B1) and Ali (B2)
- Emotional Atmosphere: Solemn
- Seating:
Figure 7: Acclimatization Session 4 - Seating Arrangement
Huma is a 23-year-old female living with her family – mother, elder sister, elder brother and
younger brother. She was brought in with complains like talking in men’s voice, playing with
human excreta, not taking medicine and shouting all of a sudden while talking.
Her issues started in 2017, after she had a break-up. She used to shout, tear off her clothes,
go to the boy’s house and create a scene. She handed over a letter to the staff with her
version of events – the contents of the letter hinted at delusions of persecution and paranoia.
No family history of any kind of psychological illness or alcohol dependence was reported.
The genogram containing her family structure is presented on the next page.
Huma has been undergoing treatment continuously since her initial diagnoses, but symptoms
had resurfaced as she refused to follow medication. Therefore, the patient and the family
were referred to the Psychiatric Social Worker (PSW) for counselling related to importance
40.
Internship Report (MCFTP001)
Page| 49
of compliance to treatment guidelines and to additionally explore any serious inter-personal
issues as the patient had previously reported instances of chaining and beating.
Figure 8: Acclimatization Session 4 - Genogram of Huma's Family
T: Good morning, Huma! How are you now?
P: I have a headache. I get tense when I see fighting. R and A fight. And B hit N on her head
while she was lying down. Even after taking medicine my nerves are hurting.
T: And, sleep?
P: It’s okay.
T: Hunger and thirst?
P: Okay.
Then the patient starts talking about things on her mind, while the counsellor patiently listens
and responds in a way that calms the patient.
P: What should I do here – I don’t understand. If I get involved in a fight, then everyone will
tell me, you are also one of them [mental patient]. It will be better if I die, the load on my
family will reduce. I’m angry with my family – they don’t let me go anywhere – even during
festivals.
41.
Internship Report (MCFTP001)
Page| 50
Then the patient deviates to an unrelated topic before coming back to her issues.
P: I like children only. Adults are stubborn. Sometimes I feel that I’ll make the children
happy, distribute kites.
The counsellor then asked some questions to confirm the status of the symptoms. While
manageable now – it was evident that the symptoms still persisted. She also mentioned that
she had a spinal injury when she was 14 and it still hurts. And, she also has sleep-related
issues since she was in 7th
. Then she was asked about medication.
T: Were you taking your medicines on time?
P: Because of side-effect I was taking half-half.
Then she was counselled that she should take the full medicine as prescribed. And, in case
there’s a problem such as side-effects, she may consult the doctor and get the medicines
changed, if required. It must be noted that the counsellor spent a lot of time to reach the
agenda of the discussion – allowing the patient time to get fully comfortable before initiating
the discussion.
Once she confirmed that she understood the importance of medication, and will follow it
properly in the future – the next issue on the agenda was discussed. The patient started
explaining the situation.
P: They keep me chained at home.
B1: She runs away from home. When we went to the police station to write a complaint, they
told us they’re not sitting free – she’s your sister take care of her yourself. That’s why we tied
her.
T: This is illegal. If she calls the police and tells them you’ll be in a problem. You shouldn’t
do this.
Then a short problem-solving discussion was done to find alternative ways to manage the
situation.
B2: Should we get the name and address tattooed on her hand?
42.
Internship Report (MCFTP001)
Page| 51
T: Yes, that should be feasible.
It seemed like a feasible solution that was discussed and finally agreed upon by all parties. P
was initially hesitant but she relented after her brothers shared their perspective – their
worries with her.
After this the T asked some more questions related to the symptoms to improve her
understanding of the situation. While this was going on, the patient mentioned another issue.
P: These people beat me. They don’t even ask what happened, whose fault is it.
T: Hitting is not acceptable. If she says something, you should discuss it – but you shouldn’t
hit her.
B1: Our mother had a heart-attack because of her. She’s also undergoing treatment.
The brothers were counselled further to ensure that any kind of confinement and violence
related issues are not repeated. After assurance was received that the behaviour would not be
repeated, the session was concluded.
There was another session later in the day with the psychiatrist. It was decided to send the
person on LoA (Leave of Absence). This was done to ensure that the patient is manageable
for the family as well as to be sure that the family does not repeat the erroneous behaviours
which they have been counselled against.
Before going on LoA she was again counselled about the importance of continuing
medication. She was also reminded that she had agreed to the request of her brothers to get
the tattoo made on her hand – however, instead of the name and address, she agreed to get
the name and phone number of her brother tattooed on her hand.
Also, the family members were again counselled against and kind of physical violence or
illegal confinement.
Upon return from the LoA, it was decided to discharge the patient as no issues were reported
by her, or by the family. She was thus, discharged with the guidance to continue treatment in
OPD.
43.
Internship Report (MCFTP001)
Page| 52
REFLECTIONS
Observing these sessions was a great opportunity for learning. Unlike the acclimatisation
sessions in the practicum for MPCE004 which were centred on similar kind of cases – young
couples facing relationship issues, these cases were very different from each other, each with
a unique set of issues under consideration.
There were several important learnings from these sessions:
1. It is very important to create an environment suitable for effective communication.
Otherwise, the patient and family members will be uncomfortable from the beginning
making it unlikely that the session will reach its potential.
2. Active listening and empathy are fundamental in establishing rapport and
understanding the patient's perspective. In the third session, the counsellor patiently
addressed the attendant's concerns, providing reassurance and education about
schizophrenia, thereby alleviating his anxieties.
3. Cultural sensitivity and language proficiency are crucial for effective communication.
Language barriers may prevent accurate expression and comprehension of symptoms
and concerns. Most of these families belonged to lower middle-class backgrounds and
using English language or even a complex sentence structure would have reduced the
efficacy of the psychiatrist/counsellor.
4. Collaboration among healthcare professionals and family members is essential for
holistic care. In the fourth session, the psychiatric social worker engaged the patient's
family in problem-solving discussions, fostering a supportive environment for
treatment compliance and addressing interpersonal issues instead of prescribing
solutions – which might have never been followed by them. Brainstorming solutions
together created a sense of shared responsibility and ownership.
5. Psychoeducation is very important. It plays a vital role in empowering patients and
families to understand and manage mental health conditions. Sessions focused on
educating family members about the patient's illness, prognosis, and treatment options
were particularly beneficial in enhancing their understanding and coping skills.
6. Addressing stigma and promoting family/community support are critically important.
In the fourth session, the counsellor emphasized the illegality and harmful effects of
44.
Internship Report (MCFTP001)
Page| 53
chaining the patient, advocating for finding better ways to address the problems
instead.
7. Use of Silence: Strategically using silence encouraged the patients and family
members to talk a lot more, thus facilitating deeper client exploration.
8. Gathering Background Information: A lot of time was spent on gathering background
details and Family-of-Origin (FOO) information for a holistic understanding. These
details influence communication styles, attachment patterns, and coping mechanisms
and also reveal important information related to the illness, the patients and the
families which more often than not turn out to be very useful for the case.
9. Client-Centric Approach: Client-centred strategies and active listening were
prioritised to encourage client expression from the beginning. This ensured that the
patients and their families felt heard and understood.
10. Use of several strategies and techniques such as validation, normalisation, ventilation,
etc. was evident in these sessions.
11. Open-ended questions were used to encourage the respondents to share information
that was important for them and talk freely.
12. Neutral Language: Even in the most complex situations the psychiatrists/counsellors
continued to use neutral language avoiding blame or judgment, which fostered a safe
space for expression.
13. Reflecting back on what clients shared demonstrated understanding and encouraged
further elaboration.
14. Collaboration within the staff: The level of collaboration amongst the psychiatrists,
clinical psychologists, psychiatric social workers, counsellors, doctors, nurses,
attendants, guards and other staff not only within their departments but even with
others - was inspirational. I believe this is one of the things which makes the institute
truly great.
Room for Improvement
While overall these sessions were great, there were some areas for improvement:
1. Quieter Environment: Noisy counselling rooms with inadequate lighting or improper
seating arrangements are not ideal at all. In the first session, despite the noisy
environment, pertinent information was gathered from the patient and her husband.
However, a quieter setting could have, perhaps, enhanced the quality of interaction.
63.
Internship Report (MCFTP001)
Page| 73
CHAPTER III: RECORD OF COUNSELLING CASE WORK 1
Peehu (pseudonym), a 13-year-old female was admitted in the hospital due to risk of self-
harm. She was already a patient of the hospital and had been diagnosed with dissociative
disorder along with behavioural issues. She and her mother were the focus of the sessions,
while her father was also involved in some sessions.
Structure advised in the ‘Framework of Case Records’ in the Internship Manual (Chadha &
Ratra, 2011) has been followed below:
REFERRAL & INTAKE
The case was referred to me by the Chief Senior Resident with the initial goals of:
1. Cutting Secondary Gains
2. Managing the ‘over-involvement’ of parents
3. Working on the parents’ attitude towards the illness (including psychoeducation)
To achieve these goals, I focused on a combination of ventilation, psychoeducation and
counselling. In addition, I also tried to build coping skills and communication and problem-
solving skills in the client.
INITIAL PHASE: REFERRAL AND INTAKE
Session 1
- Aim: Intake of the patient
- Date:
- Duration: 15:00 – 16:00 (1 hour)
- Participants: Peehu (Patient), Anya (Mother/Attendant) and Ahmed (Father)
- Emotional Atmosphere: Anxious
- Seating:
64.
Internship Report (MCFTP001)
Page| 74
Figure 9: CW1 Session 1 - Seating Arrangement
Patient’s issues started last year after she was admitted due to a self-harm attempt. After this,
behavioural issues and dissociative convulsions only got more worse. The reason for current
admission was an incident in school after which she refused to go to school unless the teacher
was removed. Since then, she has been having dissociative episodes.
Assessment of the individual was performed in terms of:
- Knowledge about illness:
o The patient was aware that she has an illness as treatment has been ongoing
for about a year. However, she was not very well educated about the illness.
o Similarly, her parents did not have a very good understanding of the illness,
and were suspected to be unknowingly contributing to the maintaining factors.
o Psychoeducation was thus determined to be one of the major objectives for
this exercise – especially, with a focus on cutting secondary gains.
- Physical/Emotional/Financial/Household routine burden:
o Considering she lives with her elder siblings and parents, there is no such
burden on her.
o Mother is under severe emotional burden as was discovered in the following
sessions – though not initially revealed by her.
o Father has normal financial burden. He was also reported to have some
medical condition because of which he just came for one session.
- Basic needs
o Basic needs are being fulfilled. No challenge was observed.
- Social support available
o Required level of social support is available to them from within the family.
65.
Internship Report (MCFTP001)
Page| 75
- Reaction of family members
o Her parents and siblings are very concerned about her and supportive of her.
- Impact of illness
o There has been severe impact of the illness. Her schooling is getting impacted
due to her repeated admissions over a short period of time.
o There was risk of harm - she reported the desire to kill herself, because of
which she had to be admitted.
To summarize, the major challenges that were identified pertained to psychoeducation about
the illness and behavioural management training for the mother who seemed to be over-
protective and contributing to the situation.
Session 2
- Aim: Detailed Work-up and Assessment
- Date:
- Duration: 14:30 – 16:00 (1 hour 30 minutes)
- Participants: Peehu (Patient) and Anya (Mother/Attendant)
- Emotional Atmosphere: Normal
- Tools Used: For this, the advised tools were used:
o Tool 2: Case History Taking of a Child/Adolescent
o Tool 3: Mental Status Examination Inventory
- Seating:
Figure 10: CW1 Session 2 - Seating Arrangement
66.
Internship Report (MCFTP001)
Page| 76
In the second session, a detailed work up was conducted with the patient. Her mother was the
informant. All these have been enclosed herewith.
Based on the detailed work up, it could be established that the respondent has a psychiatric
disorder – Dissociative Disorder marked by Dissociative Convulsions F44.5 as per ICD 10
(World Health Organisation, 1993).
During counselling emphasis was on psychoeducation for the mother and psychoeducation,
coping strategies and skill-development (focused on problem-solving and communication
skills) for the patient.
In addition, a three generation Genogram was also created while taking the case history. It
was found that the mother is currently recovering from a psychological illness, while father
developed some kidney related ailment. Patient’s eldest sister went missing at around 1-2
years of age, most probably kidnapped by some child traffickers. Her second eldest sister was
a victim of rape and then forced marriage – leading to multiple court cases.
Figure 11: CW1 - Genogram of Peehu's Family
67.
Internship Report (MCFTP001)
Page| 77
INTERVENTION ADOPTED
MIDDLE PHASE: INTERVENTION
Session 3
- Aim: Ventilation and Psychoeducation Session for Father
- Date:
- Duration: 10:00 – 11:00 (1 hour)
- Participants: Ahmed (Father)
- Emotional Atmosphere: Concerned
- Seating: The session was conducted walking around in the SOF gallery where the
patient was initially staying before moving to the ward.
Considering what the family has been through it was important to give them an opportunity
to ventilate. The first session was organised with the father – he was given an opportunity to
ventilate while I simultaneously focused on exploring his understanding of the illness,
underlying issues and family history.
He started by narrating the story of his elder daughter’s fate:
A: In 2019, before Covid the family was invited by my relatives, who laced the food with
drugs and raped my elder daughter and made her videos. Before that they had proposed her
marriage with their relative who is 10 years older – which was declined by us, as we wanted
her to first complete her education.
We did not suspect any foul play when they woke up next morning, but daughter’s
behaviour had changed completely after coming back. She started remaining quiet and to
herself. We tried to ask her but she did not tell. Then one day we found a feature phone with
her – when we question then she told us what happened.
We filed a POCSO case in court. Then they again proposed marriage to finish the
case, but we declined. Then during lockdown, I got stuck in my village – where I had gone
for some work. They somehow coaxed and threatened and married the daughter with him.
Then they brainwashed her in a way that she sided with them and filed a case on us.
68.
Internship Report (MCFTP001)
Page| 78
In court, compromise was reached that the child will stay with them – but they will
send her to school. But later they stopped. Now she’s 18 and has a daughter. She says once
the daughter grows up, she will leave them. Now she’s beginning to understand her mistake.
In 2021 her cousin had come from Dubai. He was very sad to see what happened to
her. When he went to meet her, they said such things and accused him in a way that the poor
guy committed suicide.
Because of this my wife has also developed a problem. Even the elder son has
developed anger issues. They were also getting treated from here.
After this the incident in school was discussed, and his perspective was found to be
reasonable – he wasn’t siding with or defending his daughter.
The father was counselled regarding various aspects including:
1. Psychoeducation: about dissociative disorder and the development of coping, stress
management, anger management and problem-solving skills in the patient.
2. Focus on change in child’s behaviour, instead of filing complaint against teachers
and ruining own relationship with them or changing schools.
3. Avoid being overinvolved and leave the child alone after ensuring she’s in a safe
place, when she’s having a dissociative episode.
This discussion indicated that the family may need some help with coping and it was
suggested for them to jointly undergo counselling and therapy. While the father agreed, this
could not be done as he was hospitalised himself due to some issue. So instead, it was
decided to focus on the patient and the attendant – the mother and daughter.
Session 4
- Aim: Ventilation and Psychoeducation Session for Mother
- Date:
- Duration: 12:00 – 13:00 (1 hour)
- Participants: Anya (Mother/Attendant)
- Emotional Atmosphere: Solemn
- Seating:
69.
Internship Report (MCFTP001)
Page| 79
Figure 12: CW1 Session 4 - Seating Arrangement
After giving the father an opportunity to ventilate, it was important to also give the mother an
opportunity to ventilate while I simultaneously focused on exploring her understanding of the
illness, underlying issues and her coping with her own psychological situation.
The history told by her remained mostly similar, some new details emerged which have
already been incorporated earlier.
Her understanding of the illness was explored, and she was psycho-educated on similar lines
as the father.
From this discussion, it was established that she had depressive symptoms, and the son
primarily had anger-related issues due to frustration and inability to do anything for his
sister when her life was destroyed. She also mentioned that husband also has anger and BP
related issues – his issues have been present since their marriage and he’s also controlling.
Husband has asked her to stop working and stay at home and take care of the kid – he’s
worried she’ll harm herself in their absence – even though this has never happened, and all
her attempts were in their presence. While the patient’s wrist had multiple scars from her
‘self-harm’ attempts, none of them appeared to be seriously harmful.
Mother was advised that she can and should continue working (after discussing with the
doctors) as the change of context would help her in dealing with some of the challenges she
was facing.
She was also advised to continue her own treatment and get the son and husband counselled
for the issues being faced by them.
70.
Internship Report (MCFTP001)
Page| 80
Session 5
- Aim: Understanding Peehu’s Perspective and Counselling her
- Date:
- Duration: 12:00 – 13:00 (1 hour)
- Participants: Peehu (Patient)
- Emotional Atmosphere: Calm
- Seating:
Figure 13: CW1 Session 5 - Seating Arrangement
The session was held with the patient to understand her perspective about the situation. The
child appeared to be caring and smart – she was even well aware of the processes of the
hospital based on what she had seen and experienced in the past admissions.
However, she had a lot of irrational thoughts and lacked the grit required to problem solve
out of difficult situations. This seemed primarily because of the parents – who themselves
lacked logic in their communication – their actions were responses to emotion.
This was leading to the symptoms of the child serving her with secondary gains, which she
figured and used it for manipulating the parents to get whatever she desired.
The parents – also because of what has happened with their two elder daughters - are
probably more amenable to manipulation and required the psychoeducation and counselling
that had been provided to them.
The patient was thus, counselled regarding the consequences of her behaviours, and it was
decided to explore her emotions further while also building skills.
71.
Internship Report (MCFTP001)
Page| 81
Session 6
- Aim: Exploring Peehu’s Emotions and Cognitions
- Date:
- Duration: 12:00 – 13:00 (1 hour)
- Participants: Peehu (Patient)
- Emotional Atmosphere: Solemn
- Seating:
Figure 14: CW1 Session 6 - Seating Arrangement
Considering the emotions and cognitions of the child were not fully explored this session was
conducted.
During the session, it was discovered that during the last admission, the patient developed a
close friendship with a girl from one of the CWC homes. She said the girl also had the same
problems as her – including anger issues but she controlled well, and also helped her to
control. She wanted to meet the girl and she thought she’d be here or she might come back.
She asked me about where she can meet the girl, I informed her that details about other
patients cannot be shared. However, I decided to use this as an example to teach her problem
solving in the next sessions and promised her that we will discuss this in the next session.
The issue of the incident in her school was also discussed. She had insight into her mistake
and when explained that she will have to make adjustments in her own behaviours if she has
a problem, the world will not always be willing to accommodate and change according to her
wishes, she understood and acknowledged that probably it would be better for her to move
out of the room instead of getting into a fight.
72.
Internship Report (MCFTP001)
Page| 82
Session 7
- Aim: Problem-Solving Skill Development
- Date:
- Duration: 12:00 – 13:00 (1 hour)
- Participants: Peehu (Patient)
- Emotional Atmosphere: Anxious (patient had a dissociative episode previous day),
then excited.
- Seating:
Figure 15: CW1 Session 7 - Seating Arrangement
Me: How are you feeling now?
P: Now I’m feeling better than before.
Then I reminded her that I had promised her we will jointly think about how to solve her
problem. She became excited about the session after hearing this.
P: Wow! I really want to find my friend!
And, so taking the example of the ‘missing’ friend, we started the session on problem solving,
starting first with formulation of the problem faced.
I continued to teach her how to solve the problems that she had, as she continued to solve this
problem further based on the information that she already had. I also explained to her what
we were doing – generalised it, so that she can apply in other situations.
73.
Internship Report (MCFTP001)
Page| 83
In the end, based on the information she had she approached the doctor – who asked her to
come and meet her in the OPD to get the missing information later. Thus, she was able to
successfully solve this problem, which also built her confidence, that she would be able to
solve any other problems that she faces.
Session 8
- Aim: Exploring Future Goals and Aspirations (Existential Therapy)
- Date:
- Duration: 10:00 – 11:00 (1 hour)
- Participants: Peehu (Patient) and Anya (Mother/Attendant)
- Emotional Atmosphere: Normal
- Seating:
Figure 16: CW1 Session 8 - Seating Arrangement
Based on the previous sessions it was clear that the child was well-meaning, and the
behavioural issues stemmed from maladaptation – of both her and her parents to the life
situation. Thus, it was felt that using the tools of Existentialist Therapy to refocus the child
towards the future might serve her well.
Thus, an attempt was made to refocus the cognitions of the child towards her future related
aspirations and goals. She mentioned she wanted to become a doctor and help the poor, and
patients like herself and her ‘friends.’
She was asked about the next steps in this direction. She mentioned about getting additional
classes to get her studies back on track, and then coaching for medical exams once she is in
class 11th
. She promised to focus towards this goal.
74.
Internship Report (MCFTP001)
Page| 84
She also got an idea that she can become a doctor and keep her friend as an associate –
nurse or attendant in her clinic.
By the end of the session, a good rapport was established, she had opened up and started
discussing various matters. She repeatedly requested for my contact details, but I had to turn
it down as advised by the SR – against the hospital policy.
TERMINATION & FOLLOW-UP
FINAL PHASE: TERMINATION & FOLLOW-UP
Session 9
- Aim: Preparing for Termination
- Date:
- Duration: 12:00 – 13:15 (1 hour 15 minutes)
- Participants: Peehu (Patient) and Anya (Mother/Attendant)
- Emotional Atmosphere: Positive
- Seating:
Figure 17: CW1 Session 9 - Seating Arrangement
During this session, progress made during the previous sessions was reviewed and areas of
further focus were identified – primarily a suggestion to consciously keep working on
developing the child’s coping strategies and skills, instead of letter her behavioural issues
grow. Decisions related to some specific issues, reached during the sessions were also
revisited.
75.
Internship Report (MCFTP001)
Page| 85
Me: Good morning! How are you feeling today?
Peehu: Much better now.
Anya [smiles and nods affirmatively – acknowledging the reported improvement]
Me: Great! Today, we'll look back on what we discussed during counselling and discuss how
to continue improving.
Both: (Nod affirmatively) Sure.
Me: Great! Let's first discuss about the illness and convulsions. Based on our discussions
what do you understand about it?
A discussion happened regarding dissociative disorder and convulsions. The basic concepts
were revisited and focus was on what they could do in case of a convulsion, and what they
could do to prevent it from happening.
Next, we discussed about Problem Solving skills and also the importance of expressive
communication between the parents and children.
Finally, we discussed the future goals and aspirations that were discussed in the previous
session and the patient was reminded of her promise to get back to her studies with full
motivation.
The mother was also reminded that she should get her own treatment done, and if necessary,
get her son and husband evaluated to see if there’s need for treatment or counselling to help
them function better.
During the termination, they were advised to meet the hospital counsellor if required.
Follow up sessions were not necessary, so no advice was given regarding them.
The patient was discharged from the hospital soon after this discussion.
76.
Internship Report (MCFTP001)
Page| 86
DIFFICULT SITUATIONS ENCOUNTERED
At the beginning of the sessions, I was slightly apprehensive because the respondent had
attempted self-harm in the past, and if anything was to go wrong there was a chance of me
being blamed, even if there was no fault of mine. But thankfully, nothing like this happened.
The patient responded well to the counselling sessions.
One unique difficulty in this case was that all the important information could not be obtained
during intake as the parents were quite guarded about it. It was only in the follow-up sessions
that they started opening up and sharing the more private details – which were critical to
understand what they were facing. However, once trust was established, and they shared,
things became a lot easier.
The medical situation of the father was also an impediment. I still believe the entire family is
in need of psychological help considering the multiple issues they have faced over the years.
However, due to this the plan to do family therapy had to be abandoned, and instead the focus
was shifted on counselling the patient and her mother – and working solely on this dyad.
BARRIERS IN COMMUNICATION AND HANDLING EMOTIONAL
OUTBURSTS
The child’s behaviour was unpredictable at times. Her cognition was quite volatile. As she
got new ideas her mind shifted. She even reneged on the commitments and promises she
made in earlier sessions.
Fortunately, I was able to handle the communication with the client reasonably effectively in
the sessions. However, there were instances where I almost ‘lost my cool’ but fortunately, I
regained composure in time to be able to manage the sessions well.
There were no emotional outbursts in the sessions as such but there was an episode of
dissociative convulsion that happened towards the end of the sessions, a day before one of the
sessions. I was myself anxious what will happen in the session – would that throw things
completely off-track. However, fortunately, I was able to convert the session into an activity
that she was personally interested in and excited about so it could be managed.
77.
Internship Report (MCFTP001)
Page| 87
REFLECTIONS
The sessions with Peehu and her family were a special learning opportunity as this was the
first chance I got to conduct a proper counselling programme for a case of dissociative
disorder. Normally, cases of dissociation are not admitted so at most one or two counselling
sessions are possible, however, due to her unique circumstances, this patient was admitted.
Initially, I approached the case with some apprehension due to the seriousness of Peehu's
situation and the guardedness of her parents. However, as the sessions progressed, I focused
on addressing the unique challenges presented by Peehu's mental health issues.
There are areas for improvement such as strengthening communication skills and strategies
for handling emotional outbursts, particularly during dissociative episodes.
Also, unfortunately, it wasn’t possible to address the family’s past trauma through family
therapy due to the father's medical condition, which necessitated a shift in focus to
counselling for Peehu and her mother. Additionally, managing Peehu's unpredictable
behaviour and volatile cognition, considering her impressionable adolescent age, required
patience during sessions.
One of my greatest achievements in these sessions was the ability to build trust and rapport
with the family members to an extent that they divulged the most private and traumatic
experiences from their past. These were details that they hadn’t even divulged to the
experienced clinical psychologists and counsellors/psychiatric social workers.
Initially, during the intake session the parents were reluctant to disclose certain crucial
details. However, as trust was established over subsequent sessions, they became more open,
allowing for a deeper understanding of the family's struggles and history.
Through a combination of psychoeducation, ventilation, and counselling, I was able to
uncover and, to a limited degree, address issues such as over-involvement of parents,
unresolved trauma, and maladaptive coping mechanisms.
Overall, the counselling experience with Peehu and her family was both challenging and
rewarding. The encouragement and the compliments received from the seniors during the
course of the internship were a great motivating factor.
111.
Internship Report (MCFTP001)
Page| 125
CHAPTER IV: RECORD OF COUNSELLING CASE WORK 2
Pari (pseudonym), a 29-year-old married female with two children having a history of
psychiatric illness was selected as the index patient for this case work along with her
husband. She was brought to the hospital as she was having anger outbursts.
There was flight risk, risk of harm to self and risk of harm to children. There were severe
inter-personal relation (IPR) issues with the husband.
Structure advised in the ‘Framework of Case Records’ in the Internship Manual (Chadha &
Ratra, 2011) has been followed below:
REFERRAL & INTAKE
The case was referred to me by the Chief Senior Resident with the initial goals of:
1. Identifying and working on the IPR issues between the husband and wife.
2. To manage the husband’s behaviour in the ward – especially with the hospital staff.
To achieve these goals, I focused on a combination of ventilation, psychoeducation and
counselling of the husband. In addition, I also tried to equip him with coping strategies.
For the couple, the focus was on identifying the root cause of the issues between them. And
working on their communication and problem-solving skills.
INITIAL PHASE: REFERRAL AND INTAKE
Session 1
- Aim: Intake of the patient
- Date:
- Duration: 10:00 – 11:00 (1 hour)
- Participants: Pari (Patient) and Ali (Husband/Attendant)
- Emotional Atmosphere: Tense
- Seating:
112.
Internship Report (MCFTP001)
Page| 126
Figure 18: CW2 Session 1 - Seating Arrangement
Assessment of the individual was performed in terms of:
- Knowledge about illness:
o The respondent was aware that she has an illness as treatment has been
ongoing for more than 12 years. However, she was not very well educated
about the illness.
- Physical/Emotional/Financial/Household routine burden:
o Considering she lives in a nuclear family with her husband and two children,
the entire burden of her household is normally on her
o Due to her illness everything has shifted to her husband, in addition to his
bread-earning responsibility. Thus, he is overwhelmed.
- Basic needs
o Basic needs are being fulfilled. No challenge was observed.
- Social support available
o Limited social support was available in the form of her parents – who are
elderly and mother is currently suffering from an infection.
o Husband’s family is maintaining distance. He was aware of her illness at the
time of the marriage and did not tell his family. Therefore, his family is not
very supportive of him in the situation and have clearly refused any kind of
support.
- Reaction of family members
o Her parents understand and support to the limited extent they can.
o Husband is very supportive, in spite of all that he had to bear in the past.
113.
Internship Report (MCFTP001)
Page| 127
o However, husband’s family is reportedly ‘scared’, as in the past, husband had
to spend some time in prison when she called the police during one of her
episodes and accused him of a POCSO crime.
- Impact of illness
o There has been severe impact of the illness.
o Their household has come to a halt due to her illness
o There was risk of harm - she reported the desire to kill herself, because of
which she had to be admitted.
o Husband has to be with her in the hospital, as there is no one else. Even the
daughter has to leave school, and be with her parents. The small boy can also
be seen playing with his sister in the ward of the mental hospital.
o Effectively the entire family is currently living in the ward.
Session 2
- Aim: Detailed Work-up and Assessment
- Date:
- Duration: 10:00 – 11:30 (1 hour 30 minutes)
- Participants: Pari (Patient) and Ali (Husband/Attendant)
- Emotional Atmosphere: Normal
- Tools Used: For this, the advised tools were used:
o Tool 1: Case History Taking of an Adult
o Tool 3: Mental Status Examination Inventory
- Seating:
Figure 19: CW2 Session 2 - Seating Arrangement
114.
Internship Report (MCFTP001)
Page| 128
In the second session, a detailed work up was conducted with her. Her husband was the
informant. In addition, a three generation Genogram was also created while taking the case
history. All these have been enclosed herewith.
Based on the detailed work up, it could be established that the respondent has a psychiatric
illness – the provisional diagnosis was Bipolar Affective Disorder (BPAD) with mixed
episodes versus a differential diagnosis of Emotionally Unstable Personality Disorder
(EUPD).
In addition, it could be established that as a consequence of the illness, and the burden that
has fallen on her husband – they have developed marital issues. An effort was also made to
understand various aspects of these issues.
Treatment for the disorder was managed by the psychiatrist using pharmacotherapy. Once the
respondent showed improvement, I focused on couple counselling with emphasis on
psychoeducation, coping strategies, problem-solving skill and communication skill
development.
Figure 20: CW2 - Genogram of Pari's Family
The application of Emotion Focused Therapy (EFT) was also explored considering the couple
was found to be in a dysfunctional ‘Attack-Attack’ cycle which has led to an impasse.
However, the issues were managed at a ‘symptomatic’ level using skill development with
limited use of selected EFT techniques considering I was still in the process of confirming the
ethicality and legality of me doing therapy.
115.
Internship Report (MCFTP001)
Page| 129
INTERVENTION ADOPTED
MIDDLE PHASE: INTERVENTION
Session 3
- Aim: Checking viability of intervention
- Date:
- Duration: 10:00 – 10:30 (30 minutes)
- Participants: Pari (Patient) and Ali (Husband/Attendant)
- Emotional Atmosphere: Solemn
- Seating:
Figure 21: CW2 Session 3 - Seating Arrangement
The objective of this session was to establish that in the week-long gap that was given, there’s
enough impact of pharmacological treatment to be able to begin counselling.
Me: “How are both of you doing?”
Ali: “There is significant improvement in the illness related issues. She’s not getting as much
angry as before. So, I’m feeling much better than before.”
Me: “That’s great! Pari, how are you feeling now?”
A brief assessment interview was done with Pari starting with the above open-ended
question.
116.
Internship Report (MCFTP001)
Page| 130
Based on the husband’s report as an informant, ward observation report from the nursing
staff and observation and interaction with Pari during the session it was clear that the
symptoms have begun to recede. And, she was now in a state where intervention could be
done. However, it was decided to give a couple of more days – just to be sure.
Me: “Pari, now we will meet day after tomorrow and discuss your illness - what it is, why it
happens, and so on. Meanwhile, if you have any questions about it, you can note them and we
can discuss them. Ali, you too.”
Session 4
- Aim: Understanding Ali’s Emotional State and Coping
- Date:
- Duration: 12:00 – 13:00 (1 hour)
- Participants: Ali (Husband/Attendant)
- Emotional Atmosphere: Calm
- Seating:
Figure 22: CW2 Session 4 - Seating Arrangement
The focus in this session was on understanding Ali’s emotional state.
The illness had taken a severe toll on Ali. He even had to spend time in prison due to a false
POCSO case filed against him by the respondent due to her illness. In spite of it he said:
Ali: “If she was okay and had done so intentionally, I would have left her. But, when I know
that she’s unwell, then how can I leave her? We have two children, who will take care of
them – what will happen to them.”
117.
Internship Report (MCFTP001)
Page| 131
During the session all his concerns were heard, including those with the hospital. He was
given an opportunity to ventilate. Attempt was made to help him recognize and express his
emotions in a healthy way. This was essential considering he had immense caregiver burden.
His feelings were validated and it was ensured that he feels this is a safe space where he can
express freely and authentically. This was essential for us to make any progress with the
marital issues.
He seemed to be coping alright in spite of the severe stress and lack of support. In the end he
was advised:
Me: “Ali, I hope you feel better about today’s session. Remember, it is very important that
you take care of yourself well. Only then you’ll be able to take care of everyone else. So, if
you feel the need for help you should reach out for your own counselling as well.”
Session 5
- Aim: IPDE Conduction
- Date:
- Duration: 10:00 – 11:00 (1 hour)
- Participants: Pari (Patient)
- Tools Used: International Personality Disorder Examination (World Health
Organisation, 1997)
- Emotional Atmosphere: Serious/Calm
- Seating:
Figure 23: CW2 Session 5 - Seating Arrangement
118.
Internship Report (MCFTP001)
Page| 132
This session was unplanned – conducted after a discussion during the ward round.
As advised by the consultant and Chief Senior Resident, IPDE screening was conducted to
completely rule out the possibility of the patient having a personality disorder. This was done
under the supervision of the psychiatrist in-charge of the case.
Copy of the responses and scoring results is enclosed along with to the field notes.
One unexpected advantage of conducting IPDE was that in a later discussion, when I crossed
the patient in the ward, she mentioned that she found the session therapeutic.
P: I felt good, after talking to you yesterday.
Thus, the assessment inadvertently contributed to improving the rapport with the patient.
Session 6
- Aim: Psychoeducation and Coping Strategies
- Date:
- Duration: 12:00 – 13:00 (1 hour)
- Participants: Pari (Patient) and Ali (Husband/Attendant)
- Emotional Atmosphere: Anxious (respondent had anger outburst just before the
session)
- Seating:
Figure 24: CW2 Session 6 - Seating Arrangement
119.
Internship Report (MCFTP001)
Page| 133
Before the session I reached out to the senior counsellors (professors) in the hospital to
understand and learn from them how psychoeducation is approached in different scenarios.
And, how specifically for someone diagnosed with BPAD.
The respondent and her husband had indicated very limited knowledge about BPAD, and
especially the role of stress as a trigger. Example:
- Pari had asked me previously “Why do I become violent sometimes, and silent
sometimes”
- Ali was concerned “Has my daughter also contracted this illness? She doesn’t behave
normally.”
Psychoeducation was done about:
- Bipolar Affective Disorder (BPAD) - nature of BPAD, symptoms, aetiology, triggers,
and treatment options;
- Its impact on the individual and the family.
- Coping strategies for managing symptoms and reducing the burden on the family
such as stress management techniques, relaxation exercises, and mood tracking were
discussed.
- We discussed how respondent and her husband can support each other effectively
during episodes. And, how the couple can communicate openly about symptoms and
develop a plan of action in case of an episode to prevent its advancement into more
serious stage.
Ali: “Thankyou sir! This information is very useful for us. If somebody had told us all these
things earlier, maybe we would never have reached this stage. And, I’m also less worried
now. May god bless you!”
Session 7
- Aim: Anger Management
- Date:
- Duration: 16:30 – 17:00 (30 minutes)
- Participants: Ali (Husband/Attendant)
- Emotional Atmosphere: Loud/Angry
121.
Internship Report (MCFTP001)
Page| 135
Me: Good afternoon, Pari. How are you feeling now?
Pari: I’m feeling better, thank you.
Ali: I’m fine, too.
Me: Great! Today we will focus on understanding and addressing some of the issues that both
of you are facing due to the illness and the consequent burden on you, Ali. It's important for
all of us to work through these issues together. Are you both comfortable with that?
Both: Yes.
Ali: It is important.
Me: Great. Pari, would you like to share what you feel about the situation?
Pari: [takes a moment to think] Well, it's really hard. Ali has to take so much stress and work
because of my illness. Sometimes, I feel like I'm useless - a burden.
Me: Thank you for sharing, Pari. Ali, how does hearing Pari make you feel?
Ali: [takes a deep breath] It's tough to see her struggle with the illness. But, I'm here for her
no matter what. We''ll get through this together. We have to do it for our children.
Me: That's the spirit, Ali. Pari, how does it feel to hear Ali's support?
Pari: [smiles] It feels good. His support feels good.
Me: It's very important that both of you support each other through this. Now, is there
something in your hearts – about each other – something that makes you angry at the other
person - that you both would like to discuss and clarify today?
Pari: Sometimes I feel he resents me for my illness – and blames me for everything that's
gone wrong.
Ali: (Nods) That is correct – I do get angry at time. It's not because I blame her. I feel
stressed by everything. I feel frustrated sometimes.
122.
Internship Report (MCFTP001)
Page| 136
Me: Thank you both for your honesty. It's important to acknowledge these feelings and work
through them together. We need to talk to each other about our feelings and tell each other
that we are there for each other.
Pari and Ali were guided through exercises and discussions aimed at rebuilding trust,
intimacy, and connection in their relationship. The atmosphere remained calm and
supportive.
Me: Today both of you were open and willing to work through these challenges together,
which is very good. And both of you told you are already feeling better. In the next sessions
we will learn some techniques that will help us even more.
Session 9
- Aim: Skill Development focusing on Problem Solving
- Date:
- Duration: 10:00 – 11:00 (1 hour)
- Participants: Pari (Patient) and Ali (Husband/Attendant)
- Emotional Atmosphere: Normal
- Seating:
Figure 26: CW2 Session 9 - Seating Arrangement
Problem-solving techniques such as brainstorming, identifying solutions, and evaluating
outcomes were shared to enhance problem-solving skills to address challenges related to the
individual's illness and its impact on the family.
Live problem-solving session was done using real-life scenarios. Example:
123.
Internship Report (MCFTP001)
Page| 137
Me: “Pari, can you share a problem that you are facing? Something because of which both of
you argue.”
Pari: “Ali has got chickens which make the entire home dirty, and noisy.”
Me: “Ali, would you like to say something about this?”
Ali: “But, eating fresh eggs is important for the health of the children. And, it would be
cheaper.
I maintained neutrality and asked them, considering both seem to make sense what can be
done to solve the problem.
Pari: “Maybe chickens can be limited to the terrace area.”
Me: “Ali, what do you think? Is that possible.”
Ali: “Yes. Absolutely!”
Me: “So what is the next step on this?”
Ali: “I need to make sure that the chickens are restricted to the terrace.”
I then asked them if this matter is resolved? They agreed. I congratulated them on
successfully resolving the issue. Then I asked them to share another example and took a
similar approach to reaching a resolution. They resolved the issue while I moderated the
conversation.
Overall, an attempt was made to strengthen the couple's ability to collaborate and support
each other in managing day-to-day stressors. Considering their situation, it is critically
important for them to collaboratively identify solutions to common problems and also
develop action plans for implementation.
Session 10
- Aim: Skill Development focusing on Communication Skills
- Date:
- Duration: 10:00 – 11:00 (1 hour)
124.
Internship Report (MCFTP001)
Page| 138
- Participants: Pari (Patient) and Ali (Husband/Attendant)
- Emotional Atmosphere: Relaxed
- Seating:
Figure 27: CW2 Session 10 - Seating Arrangement
This session was focused on helping them identify ineffective communication patterns such as
persistent blaming and interrupting and teaching them techniques to improve their
communication.
I encouraged them to practice active listening and showed them how assertive
communication can be used to express needs and concerns constructively.
Me: “Hello, both of you! How’re you feeling now?”
Pari: “Much better.”
Ali: “I’m fine.”
Me: “Great! Now, in our previous sessions we have discussed about some of the issues that
you focus in communication. Today, we'll try to develop skills to help you improve the
connection with each other.”
Both: (Nod) Sure.
Me: Have you noticed any specific patterns in your communication when disagreements
arise?
126.
Internship Report (MCFTP001)
Page| 140
TERMINATION & FOLLOW-UP
FINAL PHASE: TERMINATION & FOLLOW-UP
Session 11
- Aim: Preparing Couple for Termination
- Date:
- Duration: 10:00 – 11:15 (1 hour 15 minutes)
- Participants: Pari (Patient) and Ali (Husband/Attendant)
- Emotional Atmosphere: Positive
- Seating:
Figure 28: CW2 Session 11 - Seating Arrangement
During this session, progress made during the previous sessions was reviewed and areas of
further focus were identified – primarily a suggestion to consciously keep working on
communication and joint decision making. Decisions related to some specific issues, reached
during the sessions were also revisited.
Me: Good morning, both of you! How are you feeling today?
Pari: Much better now.
Ali: Me too.
Me: Great! Today, we'll look back on your journey in counselling and discuss how to
continue improving.
127.
Internship Report (MCFTP001)
Page| 141
Ali: We feel much better. Communication is much better.
Pari: (Nods) I agree. Being able to express myself without getting so frustrated has made a
big difference.
Me: Great! Let's reflect on some of the coping strategies, problem solving techniques and
communication techniques we covered.
We reviewed techniques like active listening, "I statements," and identifying triggers that
were shared with them in the previous sessions. They discussed specific situations where
these skills were helpful.
Ali: Active listening exercise really helped. Now I wait for what Pari is saying before
replying.
Pari: (Smiling) "I statements" help me express my needs without sounding like I’m blaming
him.
Me: Great! Now, let's create a relapse prevention plan. What are some early warning signs
you've identified for Pari's symptoms?
They discuss the symptoms and then Pari and Ali brainstorm what they can do, and
scheduling appointments with the psychiatrist if necessary.
Me: Great! Remember, communication is very important. Let each other know if you're
feeling overwhelmed or need support.
Both: Yes, we will.
Me: Good.
Ali: Thank you so much for everything. We feel much more comfortable – like we can
handle things.
Pari: Yes, thank you.
128.
Internship Report (MCFTP001)
Page| 142
Me: You’re welcome. But, remember, we were able to make progress only because both of
you put in the effort. If you continue doing that things will continue to improve. And, in case
you feel the need meet the hospital counsellor when you come for follow up in the OPD.
(Session Terminated)
During the termination, they were advised to meet the hospital counsellor for counselling
follow up sessions, if required, when they come for treatment follow up in the OPD.
Session 12
- Aim: Follow Up
- Date:
- Duration: 10:00 – 11:00 (1 hour)
- Participants: Ali (Husband/Attendant)
- Emotional Atmosphere: Relaxed
- Seating: NA - the session was held outdoors.
Post-termination, a follow up session was held with the husband before their discharge from
the hospital. Several aspects were covered:
- Psychoeducation: The information conveyed during the earlier session on
psychoeducation was reiterated. He had several doubts and questions, especially
related to alternative schools of medicine. The questions were either answered or, in
case of alternative medicine he was advised to discuss with the relevant experts.
- Anger Management: Both for himself and the patient.
- Supportive Therapy for him: He was also advised to seek counselling for himself if he
feels he is unable to cope with the stress and the challenges that he is facing.
He reiterated his worries about his daughter that were discussed earlier – he mentioned
several ‘symptoms’ that he had noticed. He was advised to note down all symptoms that he
feels are there, and discuss with the psychiatrist when he brings the patient to the OPD next
time.
The patient was discharged from the hospital soon after this discussion as they wanted to be
at home to celebrate Eid.
129.
Internship Report (MCFTP001)
Page| 143
DIFFICULT SITUATIONS ENCOUNTERED
At the beginning of the sessions, I was slightly apprehensive because the respondent had a
severe psychiatric illness which significantly complicated the process. But thankfully, she
responded well to the pharmacological treatment. I had to give adequate time for this to
happen. However, once there was improvement - during the sessions – I just had to be
mindful that I don’t trigger her in some way, and there were no issues.
Additionally, the family had a severe resource crunch with negligible social support.
However, the respondent and her husband have developed a significant degree of
independence, so it wasn’t a major challenge.
Apart from these there were instances of anger outbursts by both husband and wife in the
ward, and I was worried things might go off track if that reaches the counselling room.
Fortunately, it never happened, and the sessions went on smoothly.
BARRIERS IN COMMUNICATION AND HANDLING EMOTIONAL
OUTBURSTS
Considering the extremely complex situation, I believe I was able to handle the
communication with the client quite effectively in the sessions. Can’t think of any examples
when things went anywhere near out of hand.
Pre-emptive measures were undertaken by me to handle communication. This was made
possible due to a proper intake exercise which enabled me to understand the issues properly.
- As I was aware of the illness and the other issues, I could adapt my communication to
minimise any chance of triggering any of them.
- The use of pauses and silence was also very useful in the process. It gave them time to
think and process before responding – continuing with the session.
- Therefore, fortunately, there were no emotional outbursts during the sessions.
REFLECTIONS
The objective of undertaking this practicum activity, was to counsel an individual/ couple
with marital and family issues, from the initial phase till termination.
130.
Internship Report (MCFTP001)
Page| 144
Accordingly, Pari, a 29-year-old married female with 2 children was selected to be the
respondent in the activity, along with her husband. The sessions with Pari and Ali were a
rewarding experience. The impact on their communication, household, and emotional well-
being was evident.
I got the opportunity to practice some of my skills and learn new things. Like
psychoeducation specific to BPAD and its impact on families. Apart from this, witnessing the
couple acknowledge their struggles and working together towards a positive turning point left
me with a sense of achievement.
The focus on communication skills training proved to be a key intervention. The role-playing
exercises and "I statement" practice allowed them to identify ineffective patterns and replace
them with more constructive approaches. This improvement in communication style was
evident in their later sessions, where they engaged in more respectful, empathetic and
constructive discussions.
Some limitations were also there considering the context - there was limited flexibility
available – example: the counselling room had a set sitting pattern (as in a doctor’s chamber)
that could not be changed. The paint/lighting of the counselling room was also quite
‘gloomy’ – another factor I could not change.
Although I couldn't delve into Emotionally Focused Therapy (EFT) fully due to ethical
limitations, the emphasis on emotional expression and validation seemed to create a
foundation for rebuilding trust and intimacy. This was evident in their body language and
interactions during later sessions. They appeared more comfortable expressing their feelings
and frustrations – and, generally, seemed better connected.
Overall, addressing the underlying mental health issue, combined with communication skill
development and support system building, proved to be successful in this case.
Witnessing their progress from the initial state of helplessness and fighting with each other to
a place of hope for the future was truly gratifying.
From a personal standpoint, the fact that I had access to senior psychiatrists and counsellors
in one of the most reputed mental health organisations of the country – with whom I could
discuss what I was doing – made sure that the process was successful!
162.
Internship Report (MCFTP001)
Page| 181
CHAPTER V: RECORD OF FAMILY THERAPY CASE WORK 3
Pooja (pseudonym), a 32-year-old married female with no children and having a serious
medical history was selected as the index patient for this case work. Her mother and husband
were the focus of the process along with her.
Structure advised in the ‘Framework of Case Records’ in the Internship Manual (Chadha &
Ratra, 2011) has been followed below:
REFERRAL & INTAKE
I got involved in this case as the mother was more comfortable talking in Punjabi. The focus
was on uncovering the issues in the family and helping family to function better.
INITIAL PHASE: REFERRAL AND INTAKE
Session 1
- Aim: Intake of the patient
- Date:
- Duration: 10:00 – 11:30 (1 hour 30 minutes)
- Participants: Pooja (Patient) and Aditi (Mother/Attendant)
- Emotional Atmosphere: Tense
- Seating:
Figure 29: CW3 Session 1 - Seating Arrangement
163.
Internship Report (MCFTP001)
Page| 182
Assessment was performed in terms of:
- Knowledge about illness:
o The respondent was currently unaware of the illness. She was referred to me
by the psychiatrists who diagnosed her as undergoing a psychiatric episode
currently.
o The family also has limited knowledge and understanding of the illness.
- Physical/Emotional/Financial/Household routine burden:
o Physically, she underwent a major surgery (kidney transplant) a few months
back. She has been advised by the doctor to abstain from sexual intercourse
for at least a year. Physical intimacy with her husband has been severely
impacted because of this.
o Financially, her husband Hitesh had taken a loan for her surgery and is
currently working hard to pay it off. So, there is immense financial pressure on
them.
▪ As Hitesh is unable to take care of her due to his work commitments
she lives with her mother.
▪ Which in turn has led to even lesser interaction between the two, which
is impacting Pooja psychologically
o Emotionally, Pooja seems to be volatile, with a lot of pent-up emotional load
as she lost her father who she was very close to at an early age, after which her
brother whom she loved and trusted, cheated them of the ancestral property
and left her and her mother on their own.
▪ Hitesh and Pooja seem to be very close. At the same time, it seems
Pooja is insecure and feels that she might lose him.
▪ She even accused her married sister of having an illicit affair with
Hitesh, which her mother clearly denied.
o Considering she lives in a joint family with her husband and his family she has
a limited regular household burden to take care of. That is not a major concern
in this case.
- Basic needs
o Pooja’s basic needs are being fulfilled.
o However, considering her brother’s cheating, her mother is in dire straits –
with no place to live or go.
164.
Internship Report (MCFTP001)
Page| 183
▪ After Pooja helped her mother to file a case in court her son started
giving maintenance which allows her to get a bare minimum roof over
her head.
▪ This is another stressor for Pooja.
- Social support available
o Husband’s family and sister’s family are very supportive.
o Husband also has friends who are quite supportive.
o Overall, we can say that there is moderate level of social support available,
that is not a major concern.
- Reaction of family members
o The family, except her brother, was found to be generally concerned and
involved in her care. They were distressed by her situation.
- Impact of illness
o There has been severe impact of the overall medical situation on their life.
o There has been no physical intimacy for a while due to medical restriction.
o Because of the modified living arrangement, the emotional intimacy has also
been significantly impacted.
o It is also resulting in several stressors as she has done severe damage, which
has resulted in the eviction of her mother from her house.
Session 2
- Aim: Assessment – Case History, Mental Status Examination and Family
Interview
- Date:
- Duration: 10:00 – 12:00 (2 hours)
- Participants: Pooja (Patient), Aditi (Mother/Attendant) and Hitesh (Husband)
- Emotional Atmosphere: Tense, Sad
- Tools Used: For this case work the advised tools were used:
o Tool 1: Case History taking of an Adult
o Tool 3: Mental Status Examination Inventory
o Tool 4: Family Interview Schedule
- Seating:
165.
Internship Report (MCFTP001)
Page| 184
Figure 30: CW3 Session 2 - Seating Arrangement
In the second session, the Family Interview Schedule was used to interview the family
members. Apart from this the case history and mental status examination tools were used to
capture the relevant information. All these have been enclosed herewith.
Based on the information obtained, a three generation Genogram was also created.
Figure 31: CW3 - Genogram of Pooja's Family
Important points that emerged in this session are as follows:
- Complications began after Pooja’s surgery as severe resource crunch happened.
- A loan was taken for her surgery, because of which Hitesh cannot stop his work, even
to take care of Pooja.
- She required comfort from Hitesh who she considers closest, but he was present even
less than before due to the financial burden of the loan upon him.
166.
Internship Report (MCFTP001)
Page| 185
- This led to multiple issues – she started suspecting he has an affair, and also became
bitter towards others, including her in-laws and her own sister – even charging her
with having an affair with Hitesh.
- This situation is further complicated as the doctor prohibited them from sexual
intercourse for 1 year after the transplant. This has impacted their physical intimacy
negatively.
- Aditi is above 60, and as she was the one to give her kidney to Pooja – she also
become quite weak. With no one else to take care of her, she had to live with Pooja –
and ended up being overloaded – as instead of being cared for, she had to take care of
her daughter.
- Because of all these complications, currently, Pooja, Aditi and Hitesh have de facto
become a family unit – as Pooja is living with Aditi and persistently refuses to go
back to her marital home, and even they’re not very keen on having her currently.
- The immediate urgent need was thus to work on this ‘temporary family unit’ and
make it functional so that they don’t end up in crisis.
- Problem solving and communication both are currently in a very bad situation. The
family needs help to bring things under control.
- It could be established from the family interview that as a consequence of the illness,
and the financial burden that has fallen on the family – significant issues have
emerged with the family heading towards dysfunctionality.
- Additionally, from the MSE it is apparent that the patient is currently undergoing a
manic episode.
INTERVENTION ADOPTED
MIDDLE PHASE: INTERVENTION
Considering the issues were not long-term systemic or structural, and had emerged from a
very clear situation, it was decided to use Brief Strategic Family Therapy to help the family.
So, as is usually the case in BSFT, during the course of therapy the focus was on working to
resolve specific challenges and build specific areas.
167.
Internship Report (MCFTP001)
Page| 186
Session 3
- Aim: Identifying Maladaptive Patterns
- Date:
- Duration: 10:00 – 11:00 (1 hour)
- Participants: Pooja (Patient), Aditi (Mother/Attendant) and Hitesh (Husband)
- Emotional Atmosphere: Collaborative
- Seating:
Figure 32: CW3 Session 3 - Seating Arrangement
M: Good morning, everyone! How are you feeling now?
P: I’m okay, thank you.
A: [sighs] It's been a tough week, but things are improving thanks to you.
M: Good to know that things are improving! [paused to emphasise the positive] Today, we
will try to understand how you interact as a family and what challenges you're facing during
interactions. And, if there are any patterns to it.
Are you all comfortable with that?
All: Okay
M: Great! So, first, are there any recurring issues or conflicts that you've noticed – any
patterns of behaviour or communication that are repeated?
168.
Internship Report (MCFTP001)
Page| 187
P: [glancing at her mother and husband before speaking] Hitesh does not have time for me,
he does not even come to meet me and sometimes doesn’t even pick my call.
H: [Sighs] I know, even I feel so. But what can I do – I have to work to pay off…
A: [Interrupting] Is money more important than me?
M: It sounds like there's a communication breakdown here. And, it’s causing tension within
your family. This is a common issue that many families face. [NORMALISATION]
P: [Nodding] Yes. We're stuck, and I don't know how to break free from it.
M: That’s alright. Our goal is to identify these patterns and stop them - and create new, more
positive patterns of interaction. We may need to learn new skills.
All nod in agreement, signalling their understanding.
M: Now, let's explore some more instances where these patterns have emerged in your family
interactions so that we can begin to work towards positive change together.
Session continues with the family members sharing their experiences and insights, identifying
maladaptive patterns and discussing how to change.
M: Our time is up for today, but I want to appreciate you all for your openness and
willingness to explore these issues together. Remember, today we have identified the patterns
– which is the first step towards change.
Session 4
- Aim: Setting Therapy Goals
- Date:
- Duration: 10:00 – 11:00 (1 hour)
- Participants: Pooja (Patient), Aditi (Mother/Attendant) and Hitesh (Husband)
- Emotional Atmosphere: Calm
- Seating:
169.
Internship Report (MCFTP001)
Page| 188
Figure 33: CW3 Session 4 - Seating Arrangement
M: Good afternoon! How’re you all doing now?
All: Okay
M: Today, we will focus is on setting clear and achievable goals for our therapy sessions.
Shall we start?
All nod in agreement.
M: Let's start by discussing what specific outcomes you hope to achieve through therapy.
What are some areas of your family life that you'd like to see improvement in?
A: I want better communication between all of us. Right now, it feels like we're not listening
to each other.
H: I agree. And, we need to find a way to manage our stress better, especially with everything
going on with Pooja's health and the financial strain it's put on us.
P: Yeah, and I want Hitesh to be with me again. I feel like I’m alone.
M: Good. These are important goals. Let's make sure they're SMART, meaning specific,
measurable, achievable, relevant, and time-bound. Example: instead of just saying “better
communication”, let's specify what it means. What needs to happened for you to feel
communication is better?
They brainstorm to answer.
170.
Internship Report (MCFTP001)
Page| 189
M: Great! Now, let's move on to the other goals – managing stress and reconnecting as a
couple. How can we make these goals SMART?
Together, the family comes up with specific definitions of these goals.
M: The goals make sense, and with your commitment and hard work, you should be able to
achieve them. Now, let's talk about how achieving these goals will improve your family
functioning and overall well-being.
Pooja, Aditi, and Hitesh reflect on the positive impact that achieving their goals will have on
their relationships, health, and quality of life. They express a sense of hope and
determination.
M: We had a productive session today. Let’s continue with the same commitment to achieve
the goals that we set today!
Session 5
- Aim: Skill Development with a focus on Communication Skills
- Date:
- Duration: 10:00 – 11:00 (1 hour)
- Participants: Pooja (Patient), Aditi (Mother/Attendant) and Hitesh (Husband)
- Emotional Atmosphere: Supportive
- Seating:
Figure 34: CW3 Session 5 - Seating Arrangement
They were welcomed and asked about the improvements they have noticed.
171.
Internship Report (MCFTP001)
Page| 190
M: "In the last session, we set goals for our therapy sessions. Today, we'll focus on
communication skills. Effective communication means being able to express yourselves
clearly and listen attentively to each other."
M: "Let’s start with the concept of Active listening - it involves paying close attention to
what the other person is saying, both verbally and nonverbally. It shows you're engaged and
want to understand their perspective."
I explained some active listening techniques
- Maintain eye contact and lean in slightly - to show interest.
- Use verbal cues like "uh-huh" or "I see" - to acknowledge you're listening.
- Briefly summarize what you hear - to confirm understanding.
- Ask clarifying questions - to make sure you grasp the full message.
Then I moved to assertive communication.
M: "Assertive communication means expressing your needs and feelings honestly and
directly, but with respect for the other person."
I explained some assertive communication techniques.
- Use "I" statements - to own your feelings, like "I feel frustrated when..."
- Focus on the specific behavior that bothers you, not the person.
- Clearly state your needs in a positive way, example, "I need some time alone to
relax."
- Be respectful of the other person's feelings and needs, but also be firm about your
own.
This was followed up with a role-playing exercise.
M: "Let's practice these skills. Imagine…”
A scenario was presented based on their situation.
M: Pooja, can you start by using active listening as Hitesh explains his perspective?"
172.
Internship Report (MCFTP001)
Page| 191
Pooja and Hitesh participated in a role-play where Pooja uses active listening and "I"
statements to express her feelings and needs. Hitesh responds using active listening to clarify
and find solutions. Feedback was given to them about areas of improvement.
M: "Great! You both are beginning to learn active listening and assertive communication.
Remember, to practice these skills regularly."
Session continues with more role-playing exercises addressing different communication
situations in the family.
M: "Remember, try practicing these techniques in your daily interactions. Notice how your
communication feels different. "
Session 6
- Aim: Skill Development with a focus on Problem Solving
- Date:
- Duration: 10:00 – 11:00 (1 hour)
- Participants: Pooja (Patient), Aditi (Mother/Attendant) and Hitesh (Husband)
- Emotional Atmosphere: Solution-focused
- Seating:
Figure 35: CW3 Session 6 - Seating Arrangement
I welcomed them and congratulated on the progress so far.
M: "Today, we’ll focus on problem-solving skills. Conflicts will arise, what matters is how
we address them constructively."
173.
Internship Report (MCFTP001)
Page| 192
I introduced a step-by-step problem-solving approach covering the following paints and
explaining them.
1. Define the problem
2. Brainstorm solutions
3. Evaluate and choose
4. Implement the solution
5. Adjust or modify
M: "Let's try this with a real situation. Pooja mentioned a struggle finding time with Hitesh.
Can we use these steps to brainstorm solutions?"
The family follows the steps, collaboratively identifying challenges and proposing solutions
like flexible timing, or date night activities that can be done at home.
M: "Great! Now that we have some solutions - what are the pros and cons of each option?"
The family discussed the feasibility and appeal of each solution using the ‘two column
approach’.
M: "Remember, communication is key. Keep each other informed about your schedules and
be flexible. If needed, in the next session, let's discuss how these solutions worked and adjust
if needed."
We discussed applying the problem-solving framework to other identified challenges.
M: "This is great! The more you practice these techniques, the better you'll be able to use
them."
Session 7
- Aim: Exploring and Restructuring Family Dynamics
- Date:
- Duration: 10:00 – 11:00 (1 hour)
- Participants: Pooja (Patient), Aditi (Mother/Attendant) and Hitesh (Husband)
- Emotional Atmosphere: Calm
- Seating:
174.
Internship Report (MCFTP001)
Page| 193
Figure 36: CW3 Session 7 - Seating Arrangement
I welcomed them and congratulated on the progress so far.
M: "We've made good progress! Today, let’s explore how your roles and responsibilities
within the family might impact communication and decision-making."
I gently guide the family to reflect on their current dynamics.
M: "Pooja, how would you describe your role in the household before your illness?"
P: "I was more responsible for household activities. I also have a YouTube channel to earn
money."
M: "And Hitesh, what was your role in these tasks?"
H: "Honestly, I wasn't as involved in the household. The women manage."
Possible traditional role orientation.
M: "Now that Pooja's health has changed, perhaps these roles need some adjustments. How
do you think a more balanced distribution of household tasks might benefit everyone?"
The discussion continued, and they agreed to a mutually convenient readjustment.
A: "I could help out more, ensuring things run smoothly."
M: "Excellent! Remember, clear communication is crucial. Discuss everyone's limitations,
strengths and willingness. It's about teamwork and mutual support."
175.
Internship Report (MCFTP001)
Page| 194
M: "This plan is just a starting point – you may have to adjust it based on needs and
circumstances. So, open communication will ensure everyone feels heard and supported."
I also explored other aspects of family dynamics, encouraging healthy boundaries between
Pooja and Aditi, greater involvement of Hitesh and greater independence and decision-
making for Pooja.
M: "These are major changes, but your commitment and love for each other will help you be
successful."
Session 8
- Aim: Teaching how to Externalize Problems
- Date:
- Duration: 10:00 – 11:00 (1 hour)
- Participants: Pooja (Patient), Aditi (Mother/Attendant) and Hitesh (Husband)
- Emotional Atmosphere: Detached
- Seating:
Figure 37: CW3 Session 8 - Seating Arrangement
I welcomed them and congratulated on the progress so far.
M: "Today, I want to introduce a technique called 'externalization.'"
I explained the concept.
M: "Instead of seeing challenges as directly connected to a person, we must view them as
something the family faces together. Imagine these as external forces impacting your lives."
176.
Internship Report (MCFTP001)
Page| 195
M: "Think of your family as a team on a journey. [USE OF METAPHOR] Sometimes, you
encounter unexpected issues – like delayed trains, lack of food or water, etc. These represent
the problems you're facing. The key is to work together as a team to solve these, and not see
them as your family member’s doing."
I asked them to identify specific challenges they face.
M: "Let's look at some problems you've faced recently. Pooja, perhaps the frustration of not
having Hitesh around as much as you like?"
P: "Yes, exactly. It makes me so sad."
M: "Hitesh, maybe the stress of managing work and family responsibilities?"
H: "Definitely. 'Work Stress' has been a problem."
We discussed externalized problems.
M: " By externalizing these problems, you take a more objective view. It's 'Work Stress' or
'Lack of Intimacy' not someone's fault. How can you, as a team, address these external
forces?"
They collaborate on strategies to overcome the externalized challenges.
P: "Maybe we should plan some time, when he is free."
H: "And setting boundaries with work emails can help."
A: "I can offer to help out more with household work."
M: "Great! Now you're focusing on strategies to solve the problems, not blaming each other."
We followed the same process for some other problems to help them practice well
considering this was a complex process.
M: "Remember, externalizing problems helps you focus on teamwork and problem-solving.
You tackle challenges together, not against each other."
177.
Internship Report (MCFTP001)
Page| 196
Session 9
- Aim: Reframing Perspectives
- Date:
- Duration: 10:00 – 11:00 (1 hour)
- Participants: Pooja (Patient), Aditi (Mother/Attendant) and Hitesh (Husband)
- Emotional Atmosphere: Reflective
- Seating:
Figure 38: CW3 Session 9 - Seating Arrangement
I welcomed them and congratulated on the progress so far.
M: " Today, we will reflect on your perspectives about your’s family dynamics."
The family was encouraged to reflect on past challenges and present improvements.
M: "Pooja, how do you view communication within the family now compared to a few
months ago?"
P: "It feels much clearer and more respectful. We actually listen to each other and try to
understand each other's perspectives."
M: "Great! Hitesh, how do you feel about the changes in how you approach disagreements?"
H: "We don't seem to get stuck in arguments anymore. We actually work together to find
solutions."
M: "Aditi, how has this impacted you?"
178.
Internship Report (MCFTP001)
Page| 197
A: "I feel less stressed and worried."
I emphasized positive changes and reframed negative interpretations.
M: "This is great! Instead of focusing on past, let's celebrate your progress in communication
and collaboration. These are all steps towards a better family."
I explored other areas where perspectives have shifted, reframing negativity and highlighting
strengths.
M: "Remember, problems will come, but now, you have the tools to navigate them
constructively. Focus on the positive changes."
Session 10
- Aim: Developing Coping Strategies
- Date:
- Duration: 10:00 – 11:00 (1 hour)
- Participants: Pooja (Patient), Aditi (Mother/Attendant) and Hitesh (Husband)
- Emotional Atmosphere: Empowering
- Seating:
Figure 39: CW3 Session 10 - Seating Arrangement
I welcomed them and congratulated on the progress so far.
M: " Today, we’ll focus on developing coping mechanisms to manage stress."
I introduced various coping strategies.
179.
Internship Report (MCFTP001)
Page| 198
M: "Stress management techniques like relaxation exercises, mindfulness practices, or deep
breathing can be very helpful."
I facilitated a discussion on individual and family coping strategies.
P: "Maybe I could try yoga or meditation to manage my anxiety."
H: "Exercise helps me clear my head. Maybe we can schedule family walks together for
some stress relief. It will also allow us to spend some time together."
M: “Great Idea”
A: "Doing paath helps me find peace."
M: "Excellent! Remember, coping strategies are unique to each person- find out what works
best for you."
I guided the family in identifying potential triggers for stress and brainstorming coping
mechanisms to address them.
M: "Once you practice and internalise these coping skills, you'll be able to better manage
challenges and maintain your well-being."
Session 11
- Aim: Enhancing Family Support Networks
- Date:
- Duration: 10:00 – 11:00 (1 hour)
- Participants: Pooja (Patient), Aditi (Mother/Attendant) and Hitesh (Husband)
- Emotional Atmosphere: Connected
- Seating:
Figure 40: CW3 Session 11 - Seating Arrangement
180.
Internship Report (MCFTP001)
Page| 199
I welcomed them and congratulated on the progress so far.
M: "Today, we’ll explore the support networks and how they can further help and strengthen
your family."
M: "Pooja, who are some people you can rely on for emotional support?"
P: "My best friend is a great listener, and didi also helps."
M: "Hitesh, do you have friends or colleagues you confide in?"
H: "I discuss all my problems with my best friend."
M: "Aditi, are there friends or family members you can reach out to for support?"
A: "My family friends live nearby and are always there for me. They have always supported
me."
M: "Great! A strong support network is very important."
I explored ways to strengthen existing connections and identify additional resources.
M: "Feel free to invite your support network for gatherings or seeking professional help if
needed. Remember, you're not alone in this journey."
Again, used journey metaphor from previous sessions.
Session 12
- Aim: Relapse Prevention and Maintenance
- Date:
- Duration: 12:00 – 13:00 (1 hour)
- Participants: Pooja (Patient), Aditi (Mother/Attendant)
and Hitesh (Husband)
- Emotional Atmosphere: Calm
- Seating:
Figure 41: CW3 Session 12 - Seating Arrangement
181.
Internship Report (MCFTP001)
Page| 200
I welcomed them and congratulated on the progress so far.
M: "Today, we will create a relapse prevention plan to maintain these positive changes."
The family was asked to identify potential challenges and triggers.
M: "Pooja, what are some situations that might lead to increased stress or communication
breakdowns?"
P: "When I’m unwell I end up doing things that makes others hate me."
M: "Hitesh, how can you support Pooja during these times, considering the communication
skills you've learned?"
H: "Active listening and offering emotional support will be crucial. I will also have to
remember that it is happening because of her illness."
M: "Aditi, how can you create a supportive environment?"
A: "I can offer help in taking care of her and managing work."
A ‘relapse prevention plan’ was created next.
M: "The plan should include communication rules, coping strategies, and when to seek
additional support and from whom."
The family formulated relapse prevention strategies.
M: "Great! By planning for challenges and staying committed to each other, you can maintain
the changes we have accomplished so far."
With this the session was concluded.
Considering the progress made by the family, it was decided that extending the sessions
further is not necessary, and they can be terminated in the next session – as originally
planned.
182.
Internship Report (MCFTP001)
Page| 201
TERMINATION & FOLLOW-UP
FINAL PHASE: TERMINATION & FOLLOW-UP
Session 13
- Aim: Termination
- Date:
- Duration: 12:00 – 13:00 (1 hour)
- Participants: Pooja (Patient), Aditi (Mother/Attendant) and Hitesh (Husband)
- Emotional Atmosphere: Reflective
- Seating:
Figure 42: CW3 Session 13 - Seating Arrangement
I welcomed them and congratulated on the progress they’ve made.
M: "Today, is our last session. During the previous sessions you've learned valuable
communication skills, developed coping mechanisms, and built a stronger support system."
We reviewed the family's progress and celebrated their successes.
M: "Pooja, you've demonstrated remarkable strength and resilience during the sessions
inspite of your medical situation. You've actively participated in therapy and learned to
communicate your needs effectively."
P: (smiles) "Thank you. I feel I can handle challenges and feel better connected to my
family."
183.
Internship Report (MCFTP001)
Page| 202
M: "Hitesh, you've shown great commitment to improving communication and being a
supportive partner. Your willingness to adjust roles and prioritize open communication has
been instrumental."
H: "Thank you! I will try to continue practicing the tools and techniques."
M: "Aditi, your support has been crucial and you are a pillar of strength for your family."
A: "I feel less stressed and more confident now."
We revisited the relapse prevention plan.
M: "Let's review the relapse prevention plan and make any necessary adjustments. "
Additionally, they were worried what if things go wrong again. I asked them to visit the
hospital and meet the doctors and counsellors, if required. (Provided resources for future.)
The session concluded with a warm and positive atmosphere.
M: " Remember, you have done great! Communication, collaboration, and support are key. "
Family members thanked and express their gratitude before the session ended.
DIFFICULT SITUATIONS ENCOUNTERED
At the beginning of the sessions, I was slightly apprehensive because Pooja had a severe
psychiatric illness which significantly complicated the process. But thankfully, there were no
issues during the sessions - I just had to be mindful that I don’t trigger her in some way.
Initially, when I started, I wasn’t sure how to progress as Pooja’s in-laws had not come to the
hospital even once to visit her. After starting I realised that currently the family setup is
entirely different – and thus, decided to focus on it.
Apart from these there were instances of anger outbursts by Pooja and breakdowns of Aditi in
the ward, and I was worried things might go off track if that reaches the counselling room.
Fortunately, it never happened, and the sessions went on smoothly.
184.
Internship Report (MCFTP001)
Page| 203
BARRIERS IN COMMUNICATION AND HANDLING EMOTIONAL
OUTBURSTS
I believe I was able to handle the communication with the client quite effectively in the
sessions as pre-emptive measures were undertaken by me to handle communication.
This was made possible due to a proper intake exercise using the provided tools which
enabled me to understand the unique situation and issues properly. As I was aware of the
illness and the other issues, I could adapt my communication to minimise any chance of
triggering any of them.
Therefore, fortunately, there were no emotional outbursts during the sessions.
REFLECTIONS
The objective of undertaking this practicum activity, was to do family therapy for a
couple/marital unit/family with marital and family issues, from the initial phase till
termination and prepare a record of the same.
Accordingly, the couple Pooja and Hitesh were selected, along with Aditi – the mother-in-
law. The sessions with Pooja, Hitesh, and Aditi were a great learning experience. It was an
opportunity for me to practice family therapy properly for the first time.
In spite of the unique challenge of a psychiatric situation, the family actively participated and
demonstrated a willingness to learn. Setting reasonable, clear and SMART goals at the outset
proved beneficial.
Developing their skills related to communication and problem-solving empowered them to
move beyond blaming each other and focus on collaboratively tackling challenges.
Restructuring family dynamics and externalizing problems encouraged them to view
challenges as problems to be solved, and obstacles to overcome together, not individual
failures.
Throughout, my grasp of Brief Strategic Family Therapy continued to improve. The approach
provided a structured framework for facilitating positive change within a short timeframe. It
185.
Internship Report (MCFTP001)
Page| 204
emphasized the importance of targeting specific goals, clear communication, and
empowering the family to become self-sufficient in managing their challenges.
There were some limitations that I faced:
- Considering the context there was limited flexibility available – example: the
counselling room had a set sitting pattern (as in a doctor’s chamber) that could not be
changed.
- The paint/lighting of the counselling room was also quite ‘gloomy’ – another factor
that I could not change.
- Considering the rapid approach taken due to time constraints, it wasn’t possible to
organise individual counselling sessions, which I believe would have been useful –
for both Aditi and Hitesh.
In the end seeing the improvements in the family filled me with a sense of accomplishment.
The effort they put in was also inspiring.
From a personal standpoint, the fact that I had access to senior psychiatrists and counsellors
in one of the most reputed mental health organisations of the country – with whom I could
discuss what I was doing – made sure that the process was successful!
This experience has further strengthened my belief in the importance of Family Therapy
which unfortunately, is currently not in use anywhere near the extent to which it should be in
the Indian context. The complex familial structures of Indian families make family therapy
even more important in the Indian context.
225.
Internship Report (MCFTP001)
Page| 249
CHAPTER VI: RECORD OF FAMILY THERAPY CASE WORK 4
Pulkit (pseudonym), a 17-year-old male was selected as the index patient for this case work.
He was admitted to the hospital after a reported attack using a knife on the sister – the sister
was scratched, though not grievously hurt. His family, including his father, mother and sister
were the focus of the process along with him. His uncle and grandfather were also part of
some sessions.
Structure advised in the ‘Framework of Case Records’ in the Internship Manual (Chadha &
Ratra, 2011) has been followed below:
REFERRAL & INTAKE
The case was initially referred/assigned to me by the Chief Senior Resident with following
goals:
1. Assess if there is imitation of symptoms from father in son
2. To manage father’s ‘over-involvement’ and interference in the treatment
3. Explore the adolescent and family’s history
4. Explore family IPR issues
However, as these goals were achieved, it was realised that there are severe issues in the
family – due to the behavioural issues of the teen, which in turn were themselves stemming
from parenting and family related issues, thus warranting family therapy.
INITIAL PHASE: REFERRAL AND INTAKE
Session 1
- Aim: Intake of the patient
- Date:
- Duration: 14:30 – 16:00 (1 hour 30 minutes)
- Participants: Pulkit (Patient) and Aditya (Father/Attendant)
- Emotional Atmosphere: Tense
226.
Internship Report (MCFTP001)
Page| 250
- Seating:
Figure 43: CW4 Session 1 - Seating Arrangement
Assessment was performed along the following dimensions:
- Knowledge about illness:
o The patient is well aware of the illness.
o The family is also well aware of the illness considering the father is also
undergoing treatment for the same illness.
o The existence of behavioural issues is also well understood by everyone, but
they haven’t been explored and understood properly before.
- Physical/Emotional/Financial/Household routine burden:
o Physically, the patient is overweight, no other issues were reported. No one
else was reported to have any issues.
o The patient was found to have severe confidence and emotional issues.
o Financially, the family is comfortably positioned.
o Household is managed by the mother, no challenges reported.
- Basic needs: No issues related to fulfilment of basic needs were reported.
- Social support available: Sufficient support available from FOOs of both father and
mother.
- Reaction of family members
o Everyone blames the patient for the behavioural issues, and while they’re
concerned for him, mostly maladaptation was observed.
- Impact of illness
o Severe: Patient’s education has stopped – he stopped going to school, and was
admitted after a reported knife attack on sister.
227.
Internship Report (MCFTP001)
Page| 251
Session 2
- Aim: Assessment – Case History and Mental Status Examination
- Date:
- Duration: 14:00 – 16:00 (2 hours)
- Participants: Pulkit (Patient) and Aditya (Father/Attendant)
- Emotional Atmosphere: Tense
- Tools Used: For this case work the advised tools were used:
o Tool 1: Case History taking of an Adult
o Tool 3: Mental Status Examination Inventory
- Seating:
Figure 44: CW4 Session 2 - Seating Arrangement
In the second session, a detailed work up was conducted with the patient. His father was the
informant. The originals have been placed in the hospital files, but copies of the tools in the
format given in the internship manual have been enclosed herewith along with the field notes.
Before the session, I had a short chat with the patient in an attempt to establish rapport with
him as he was found to be reserved in the previous session. I wanted him to feel comfortable
in expressing freely during the session, even though the focus was on the father while getting
the case history.
Based on the detailed work up, it could be established that the respondent has a psychiatric
disorder – Obsessive Compulsive Disorder which is under F42 as per ICD 10 (World Health
Organisation, 1993). Conduct Disorder, which was being explored for the current admission,
could not be established conclusively at this stage as there was threat of harm, but no actual
228.
Internship Report (MCFTP001)
Page| 252
harm done. Even intent of harm could not be conclusively established from the video
‘evidence’ provided by the father. He mentioned there were more videos, which he was asked
to arrange. [The videos were never arranged.]
In addition, the father seemed to be authoritarian and was found to be highly critical of the
patient. The patient was defiant in his behaviour towards father. This was not generalised
towards other authority figures – such as doctors and hospital staff. No one reported any
issues about him. However, several complaints had been received about father’s
argumentative behaviour.
It was decided to proceed and explore the family more through a family interview.
Accordingly, the father was advised to bring the mother and the sister for the next session.
In addition, a three generation Genogram was also created while taking the case history. It
was found that the father also has OCD and is taking ayurvedic medication for the same. No
other issues were reported.
Figure 45: CW4 - Genogram of Pulkit's Family
Session 3
- Aim: Assessment – Family Interview
- Date:
- Duration: 15:00 – 16:00 (1 hour)
229.
Internship Report (MCFTP001)
Page| 253
- Participants: Pulkit (Patient), Aditya (Father/Attendant), Mala (Mother) and Sonam
(Sister)
- Emotional Atmosphere: Calm
- Tools Used: For this case work the advised tools were used:
o Tool 4: Family Interview Schedule
- Seating:
Figure 46: CW4 Session 3 - Seating Arrangement
In the third session, the Family Interview Schedule was used to interview the family
members. All these have been enclosed herewith.
Important points that emerged in this session are as follows:
- Father has OCD. Son has been diagnosed with OCD. He is currently admitted due to
behavioural issues suspected to be Conduct Disorder or ODD – but none of these have
been established so far.
- There is sufficient social support available – from family and friends.
- Father is authoritarian and dominating. He holds power due to his financial role and
as head of family. However, the teenage children are rebelling.
- Family functioning is poor resulting in behavioural issues in one child and strife in the
other as well.
- Problem Solving in the family is quite poor – it is not logic driven – father dominates
with his perspectives.
- Communication in the family has broken down – there is lot of blaming and
accusation. They seem to be significantly disengaged from each other.
231.
Internship Report (MCFTP001)
Page| 255
improvement of the Family System. Selected Cognitions were also targeted during the
sessions.
Session 4
- Aim: Explore Family Dynamics
- Date:
- Duration: 15:00 – 16:00 (1 hour)
- Participants: Pulkit (Patient), Aditya (Father/Attendant), Mala (Mother) and Sonam
(Sister)
- Emotional Atmosphere: Strained
- Seating:
Figure 47: CW4 Session 4 - Seating Arrangement
This session was conducted to understand the family dynamics, and complete and confirm
aspects of the family history with the other family members.
Me: Good morning, everyone! How are you feeling now?
All: Okay.
Me: Good! Today, we will try to understand how your family interacts and functions. And, if
there are any patterns to it. Are you all comfortable with that?
All: Okay
Me: Great! But before we begin, I need to verify some details with you.
232.
Internship Report (MCFTP001)
Page| 256
Verification of details was carried out. The original timelines reported by the father were
found to be erroneous, and consequently, the hypotheses about imitation of OCD symptoms
by the patient were rejected.
The parents were married in 2004. Mother reported observing OCD symptoms in the father
soon after marriage – however, treatment was not started. He used to repeatedly check locks,
count notes, etc.
Patient’s symptoms were first observed in 2014 and treatment was started with a local doctor
in 2015. The father’s treatment was started 1-2 years after that. OCD symptoms of the patient
are currently under control and behavioural issues and perceived intent to harm others is the
reason for admission.
Post the verification of these facts, the relationship dynamics, interaction patterns etc. were
explored. During this conversation, the matter of the knife-attack surfaced. Sister’s injury
from the knife attack was evaluated – they were shallow, minor cuts – harmless, not
stabbings. When asked about it, patient said:
P: Why will I stab hard, I don’t want to go to jail.
He was educated that even this was sufficient if his sister wanted to take legal action against
him – or call the police. He was also counselled that he will soon be 18 – and legally the
implications could be much more severe.
During the session, several severe IPR issues emerged – mostly with the father at the centre
of the situation. Therefore, it was decided to focus on the father in the next session.
Session continues with the family members sharing their experiences and insights, identifying
maladaptive patterns and discussing how to change.
Session 5
- Aim: Developing Emotional Expression
- Date:
- Duration: 12:00 – 13:00 (1 hour)
233.
Internship Report (MCFTP001)
Page| 257
- Participants: Pulkit (Patient), Aditya (Father/Attendant), Mala (Mother) and Sonam
(Sister)
- Emotional Atmosphere: Solemn
- Seating:
Figure 48: CW4 Session 5 - Seating Arrangement
Me: Good afternoon! How’re you all doing now?
All: Okay
In the last session several severe IPR issues emerged – mostly with the father at the center of
the situation. Therefore, an attempt was made to help the father communicate better. He was
asked to focus on two things:
1. Try to put his emotions into words and convey them explicitly to the concerned
person.
2. Try to understand the emotions and the point of view of the other person.
As an example, to demonstrate the issue and to help him understand how to resolve it, the
father-daughter dyad was selected. The father-daughter dyad was selected intentionally with
the idea of making it clear to the father that his behaviour is the root cause of the issues
currently present in the family.
The daughter was then asked:
Me: Do you currently have any major ongoing issue with your father?
D: He doesn’t allow me to take the scooty to the college – asks me to go in a bus.
234.
Internship Report (MCFTP001)
Page| 258
Both the sides, even the mother was allowed to put forth their points of view. In the end it was
established that the college is barely a kilometre from their home. The daughter is even
comfortable walking to the college, but the father becomes anxious about her security and
insists that she takes the bus – she does not want to do it because of the unnecessary waiting
time. Taking the scooty instead is more comfortable for her. The issue was being discussed at
home for over a month, and was currently at an impasse
Both the parents were demonstrated how, in a few minutes, we were able to reach at the core
of the issue.
Me: Great! Now, at least we know the core of the issue. The core is not the scooty – the core
is a father’s anxiety about her daughter’s security – he is concerned about her. Have you ever
told your daughter how concerned you feel?
A: No. But I have told her not to take the scooty.
The discussion continued and after a lot of to and fro, the family ultimately reached a
conclusion that:
- The father would immediately help both the children get a learner’s licence, so that
they can start learning to drive.
- The daughter would either go to the college with her father, or walk with her brother,
or take the bus for the next one year.
- After that she would be allowed to take the scooty to the college.
The family was thus shown how expressing their emotions will help the other person
understand their perspective and concerns better, and thus, help in the process of reaching
amicable solutions.
The family was also counselled in no uncertain terms that they are at a stage where they need
to decide which of the two paths they want to take – one path goes to them separating and
hating each other – the direction in which they’re currently headed. And the second one goes
to them developing a healthy relationship like a normal family and becoming a happy loving
family. This is possible today, but the option may not be available sometime soon in the
future.
235.
Internship Report (MCFTP001)
Page| 259
Session 6
- Aim: Exploring and Improving the Mother-Son and Sister-Brother dyads
- Date:
- Duration: 15:00 – 16:00 (1 hour)
- Participants: Pulkit (Patient), Aditya (Father/Attendant), Mala (Mother) and Sonam
(Sister)
- Emotional Atmosphere: Curious
- Seating:
Figure 49: CW4 Session 6 - Seating Arrangement
Picking up from the last session, they were asked if they were ready to put in the effort to
improve their family’s situation. They expressed their eagerness to improve the situation and
stated they were willing to do anything to make it happen.
Me: Good! So today we will discuss Pulkit’s relation with Mala and Sonam.
So, I proceeded with further investigating the intra-dyad dynamics of the mother and sister
with the patient, to understand what was driving the issues and to improve them.
Me: First, let’s discuss about the relation between Pulkit and Sonam. Pulkit what happened
that made you attack her? [NOTE THE AVOIDANCE OF WHY]
P: She says bad things about me and mocks me – calls me useless, failure, loser...
S: I just do it because I get irritated with what is going on. I don’t mean to hurt him.
236.
Internship Report (MCFTP001)
Page| 260
It was understood that while the sister got irritated with what was going on and often teased
her brother, she did not have ill feelings for her brother. And, she readily apologised when
she was shown her mistake in terms of the teasing. The patient was however sceptical about
whether she genuinely cares about him and means what she’s saying.
P: She’s saying just like that. She hurts me intentionally. She’s not genuinely sorry.
They were counselled that once their parents are gone, they will have to take care of each
other, and that nobody would understand the hardships they’ve gone through like they can.
They were encouraged to spend more time together doing activities of common interest or
mutual benefit to start working on their relationship. Example: patient could walk the sister
to her college, as discussed in the previous session.
After both brother and sister seemed to have reached a stage where they could communicate
openly on matters, we moved to the patient and mother dyad:
P: I love my mom. And I also love everyone in her family.
M: Yet, he abuses me and says ill things about me.
Patient did not have an answer to this and promised:
P: I will not repeat such behaviour in the future. But she mocks me, I can’t talk freely to her –
I feel bad. But I love her.
Me: Can you give an example of when she mocked you?
P: I told her about a girl I liked, and she rejected me. My mom mocked me and insulted me
instead of helping me.
The mother was counselled to become the sounding board for her son and listen to his
feelings, and not mock him. She was apprised of the importance of her role in this situation
where the child is heading towards delinquency.
In this session it was established that while the mother-son and brother-sister dyads are not
fully functional, they need minimal counselling and guidance to normalise.
237.
Internship Report (MCFTP001)
Page| 261
Perhaps, this session itself could be enough for it.
Session 7
- Aim: Exploring and Improving the Mother-Daughter and Husband-Son Dyads
- Date:
- Duration: 12:00 – 13:00 (1 hour)
- Participants: Pulkit (Patient), Aditya (Father/Attendant), Mala (Mother) and Sonam
(Sister)
- Emotional Atmosphere: Solution-focused
- Seating:
Figure 50: CW4 Session 7 - Seating Arrangement
I welcomed them and congratulated on the progress so far.
Me: Today, we’ll discuss about Aditya and Mala’s relation and Mala and Sonam’s relation.
Let’s start with Mala and Sonam. Sonam what would you like to say about your relation with
your mother?
S: She is very nice and caring. I have only one issue that whenever something happens, she
sides with papa. Like, in the case of Scooty.
M: [nodded and smiled embarrassedly]
The mother was counselled to be more rational and play the role of a neutral moderator
when conflict like situations happen at home. I asked her:
Me: When you were a teacher and conflict happened in class, did you side with one person?
238.
Internship Report (MCFTP001)
Page| 262
M: No. I remained neutral – unless I knew one person was clearly wrong.
She was advised to take a similar approach at home – draw into her education and
experience as a teacher for this. Again, it was found that the relation between the mother and
daughter didn’t need much work, just some fine-tuning perhaps.
Next, we moved to the husband-wife dyad. Considering husband’s behavioural issues were
already covered in detail in the earlier session while exploring the father-daughter dyad,
these weren’t focused on too much to prevent him becoming defensive.
However, when the wife was asked how she feels because of the atmosphere at home:
M: Sometimes I feel suicidal. I have never taken any step in that direction. But I do get the
thoughts.
This statement seemed to be a shocker for the husband and a major turning point in the
family therapy. The gravity of the situation seemed to have finally dawned on him, and all his
defences seemed to have been breached/broken. Finally, it was clear to him that everyone in
his family of procreation had issues because of him:
A: So, what should I do? Should I leave home – leave them alone – and live separately?
The tone indicated that the statement was nor defensive or sarcastic. He was suggested that
instead of separating permanently, he should work on building communication and problem-
solving skills. And for the time being, for the times when there are issues at home and he
wants to move away, he may want to explore other temporary and healthy options such as
Vipasana – which will allow him a short break and time for introspection.
In addition, he was advised to explore alternative treatment options beyond the currently
ongoing Ayurvedic treatment – possibly starting treatment for OCD and irritability at IHBAS
itself.
Session 8
- Aim: Exploring Patient’s Emotions and Thoughts
- Date:
- Duration: 15:00 – 16:00 (1 hour)
239.
Internship Report (MCFTP001)
Page| 263
- Participants: Pulkit (Patient)
- Emotional Atmosphere: Calm
- Seating:
Figure 51: CW4 Session 8 - Seating Arrangement
Considering the sessions held so far, it was important to evaluate the progress made in terms
of the behavioural issues for which the family had primarily come. It was important to check
the emotions and cognitions of the patient to determine any future risk. Considering a very
good working relationship had been established with the patient, this was also an opportunity
to explore details or aspects which have not surfaced so far – details he might not have
shared earlier.
I welcomed the patient and checked with him how he’s feeling now. After which the
discussion was steered towards his issues and concerns. A number of previously unexpressed
problems were stated by the patient which ended up proving that taking an integrative and
solution-oriented approach in this case was the correct decision – as the other approaches
would have required significant course correction.
The concerns stated by him included:
- Complete lack of a social circle even within the family.
- No guidance on studies – he was confused what to do and what stream to take – he
took medical in 11th
but failed, primarily because he didn’t study.
- He has the desire to go and live with his maasi and her family because they treat him
with love and also go for a lot of trips and vacations. However, they have refused any
240.
Internship Report (MCFTP001)
Page| 264
such arrangement even when his parents expressed that they are willing to bear all
expenses – they are apparently aware of and fearful of the patient’s behaviour.
- He was bullied/made fun of in school – because he used to obsessively question about
things, which has severely impacted his confidence in social interactions.
- Being a teenager, he is also interested in sexual experiences. However, considering
the lack of a social circle he is unable to develop any relation. He resorts to watching
porn on the mobile for hours and masturbating.
- In a related incident, once he was encouraged by his classmates to masturbate in
class. He did it, but was caught and punished. This led to further teasing and bullying
in school.
These different concerns were discussed with the patient and he was counselled about them.
Primarily:
- He was advised to join back regular school in 2024 considering the importance of
developing social skills and a social circle. In the interim, he was advised to practice/
study PCM, primarily Maths, so that he can be comfortable when the school resumes.
Based on his comfort at that point of time, he was advised to go with PCB +M or PCB
+ PE as he preferred.
- He was also advised to reflect about what he would want to become in life and align
his stream to that.
- In addition, he was advised to pick up some kind of physical exercise – gymming or
martial arts to work on his physical health, currently bordering on obese. He was
advised to do it in the form of classes, where he can additionally develop a social
circle.
In the previous sessions he had already been counselled about his behavioural issues. The
point was briefly touched and the suggestions reemphasized in this session.
Session 9
- Aim: Addressing Dysfunctional Cognitions through Psychoeducation about
Parenting
- Date:
- Duration: 12:00 – 13:00 (1 hour)
241.
Internship Report (MCFTP001)
Page| 265
- Participants: Aditya (Father/Attendant) and Mala (Mother)
- Emotional Atmosphere: Serious
- Seating:
Figure 52: CW4 Session 9 - Seating Arrangement
In this session, the focus was on addressing some dysfunctional cognitions identified in the
parents during the previous sessions which were stemming from their views about parenting
which was traditional disciplinarian.
I greeted them and asked how they were.
Me: We have previously discussed about parenting. Today, we'll get into detail and discuss
parenting styles and their impact on children. As we have discussed before, it seems your
current approach might be contributing to Pulkit's behavioural issues.
They were explained the concept of parenting styles, especially authoritarian.
Me: Therefore, it is important for you to switch to democratic and authoritative parenting
styles that encourage communication and respect for the adolescent child.
M: I think you’re right. Being too strict with him might have led to the problems. Even
Sonam seems to be developing some behavioural issues.
A: Yes. It's hard to change, but I'm willing to do anything for the sake of my children.
I appreciated their willingness to change at this age and life stage. And even more
importantly, for allowing me - an outsider to guide them on a matter as sensitive and
personal as parenting.
242.
Internship Report (MCFTP001)
Page| 266
Session 10
- Aim: Skill Development focusing on Expressive Communication and Joint
Problem Solving
- Date:
- Duration: 15:00 – 16:00 (1 hour)
- Participants: Pulkit (Patient), Aditya (Father/Attendant), Mala (Mother) and Sonam
(Sister)
- Emotional Atmosphere: Calm
- Seating:
Figure 53: CW4 Session 10 - Seating Arrangement
Considering the critical importance of emotional expression and joint problem solving in this
case, a focused session was done to review the impact of the earlier discussions and practice
some more.
Me: In previous sessions we have discussed and practiced emotional expression and problem
solving. Today, we'll practice some more and also learn communication skills like "I"
statements and active listening. This will help you express needs clearly and understand each
other's perspectives.
First, feedback was collected from them about the impact of the previous session. And their
questions and concerns were addressed. Once it seemed they were comfortable, "I"
statements and active listening were demonstrated through examples.
Me: Now, let's practice! Let's say Pulkit wants to watch a movie with a friend, and Aditya is
hesitant. How will this situation be resolved?
243.
Internship Report (MCFTP001)
Page| 267
Family practices using the hypothetical scenario. Feedback and suggestions were given to
them to enable further improvement.
Me: Great! Now, let's explore problem-solving together.
The problem-solving process was explained to them. In addition, the importance of
externalising problems was highlighted.
Family was asked to identify a real problem that they were facing currently. After which they
brainstormed solutions. They were guided in externalising the problem and then following a
collaborative approach to solve the problem using the problem-solving process.
Session 11
- Aim: Reinforcing Improvement in Family Dynamics.
- Date:
- Duration: 15:00 – 16:00 (1 hour)
- Participants: Pulkit (Patient), Aditya (Father/Attendant), Mala (Mother) and Sonam
(Sister)
- Emotional Atmosphere: Reflective
- Seating:
Figure 54: CW4 Session 11 - Seating Arrangement
This session was scheduled with the objective of evaluating the improvements in family
dynamics after the first 10 sessions, as well as reinforcing the improvements so that the
family can move closer to normality.
244.
Internship Report (MCFTP001)
Page| 268
Me: The first thing we will do today is to evaluate how far we have come after 10 sessions.
What are the improvements we can see in our family dynamics?
The family members shared their perspectives about the improvements they have noticed
after the past 10 sessions. Overall, significant improvement was reported – the number of
times there were arguments between them had significantly reduced.
Next, we moved to discussion about the roles in the family.
Me: Next, let's look at the roles each member plays within the family. Are these roles helpful
or hindering communication?
Family discusses individual roles and how they interact. Power imbalances were noticed and
adjustments suggested.
Me: Pulkit, you mentioned feeling like you don't have a voice. How can we ensure that you
feel heard?
The patient shared his perspective. After which the family discussed ways to give everyone an
opportunity to express their opinions and feelings.
The importance of joint decision making and explaining the rationale behind decisions was
reemphasized.
TERMINATION & FOLLOW-UP
FINAL PHASE: TERMINATION & FOLLOW-UP
Session 12
- Aim: Reframing Perspectives Positively Before Termination
- Date:
- Duration: 10:00 – 11:00 (1 hour)
- Participants: Pulkit (Patient), Aditya (Father/Attendant), Mala (Mother) and Sonam
(Sister)
- Emotional Atmosphere: Calm
- Seating:
245.
Internship Report (MCFTP001)
Page| 269
Figure 55: CW4 Session 12 - Seating Arrangement
Considering the family was at a breaking point at the beginning of the sessions, the distance
they had covered in the short span of time was phenomenal. It was important to celebrate this
victory so that they have a sense of achievement. This shared success would contribute
further to their reintegration and further improvement in their family dynamics.
Me: Today, let's reflect on our progress so far. When we had the first session, the
communication was strained, there was a lot of conflict and there seemed to be no end to the
problems.
Followed by highlighting their specific improvements in communication, problem-solving,
and emotional expression – congratulating them on their successes.
P: I'm very happy to see how far we've come. [Others nod in agreement.]
A: It's been a challenging journey, but I'm proud of how much we've grown as a family.
Me: These changes took effort from everyone – well done! Now, let's reevaluate the situation
and compare it to when the sessions started.
Family remembers the negative aspects and realises the positive changes achieved. Overall,
as desired, the session ended with the family feeling positive about their achievements during
the sessions so far. Thus, they were now ready for termination.
Session 13
- Aim: Termination
- Date:
247.
Internship Report (MCFTP001)
Page| 271
Family members thanked and express their gratitude before the session ended. They asked for
my personal phone number, but I had to decline the request as per the hospital protocol.
DIFFICULT SITUATIONS ENCOUNTERED
There were two major difficult situations faced during these sessions.
First was at the outset. It was reported that the patient had attacked the sister and attempted to
stab her with a knife. The patient had been admitted on this basis – risk of harm to others.
However, fortunately I probed further about this during the intake and after watching the
videos it was clear that there was absolutely no intent to harm at all.
Second was the father’s denial and resistance to the suggestion that the issues could stem
from his personality and behaviours, specifically the parenting style. “Hum bhi to aise hi pale
bade hain. Hamaare maa-baap bhi aise hi pitai kiya karte the hamari.” However, the fact
that I maintained neutrality during the session, built his trust in me.
And, just then, there was a breakthrough when his wife mentioned about suicidal ideation.
That was the shock that made him genuinely reflect about what was going on.
So, fortunately, I was able to manage both the difficulties and the sessions went well.
BARRIERS IN COMMUNICATION AND HANDLING EMOTIONAL
OUTBURSTS
The biggest barrier in communication was the patient’s reserved nature in the beginning. He
was unwilling to reveal anything. However, after spending considerable amount of time in
establishing rapport, he started trusting me – enough to share the most personal details which
he hadn’t even shared with the psychiatrists, clinical psychologists and counsellors who had
worked on his case so far.
There were several emotionally charged situations, such as the point where the wife
mentioned about her suicidal ideation, or when in the one-on-one session the patient
mentioned about how his friends coaxed him to masturbate in class, then got him caught and
then mocked and bullied him. However, fortunately, the situation remained in control and
there were no emotional outbursts during the sessions.
248.
Internship Report (MCFTP001)
Page| 272
REFLECTIONS
The reason I selected this case for the report was because this was probably the most
satisfying case that I handled during my internship period. Overall, it was challenging yet
rewarding, and valuable insights have been learnt from the experience.
Despite initial tensions and resistance, the family demonstrated a genuine commitment to
addressing their issues and improving their relationships. This willingness to collaborate
allowed for meaningful progress to occur throughout the sessions.
The eclectic approach utilized proved effective in addressing the complex nature of this
family's challenges. By drawing from various therapeutic modalities, such as cognitive-
behavioural techniques, psychoeducation, and family systems theory, intervention could be
tailored to suit the family's unique needs.
This integrative eclectic approach made it possible to develop a holistic understanding of the
family dynamics and provided a comprehensive framework for intervention.
However, there were also limitations encountered during the therapy process. While
significant progress was made within the limited session timeframe, there were aspects that
could have been explored in more depth given additional time. Additionally, certain issues,
such as individual mental health concerns, were kept beyond the scope of the family therapy.
Despite efforts to foster open communication and collaboration, there were moments of
resistance and defensiveness from some family members. Addressing these barriers required
delicacy and patience, and at times, progress was slower than anticipated. However, it
worked out fine in the end.
Conducting these sessions was enriching – it deepened my skills in family therapy:
facilitating dialogue, managing conflicts, and promoting positive change within familial
systems.
Overall, while there were challenges and limitations encountered, the experience of working
with this family was full of learning and contributed immensely to building my confidence as
a family therapist.
292.
Internship Report (MCFTP001)
Page| 321
CHAPTER VII: REFERENCES
Aims & Objectives Of IHBAS. (2024). Retrieved April 19, 2024, from Institute of Human
Behaviour and Allied Sciences: https://ihbas.delhi.gov.in/ihbas/aims-objectives-ihbas
American Psychological Association. (2010). Ethical Principles of Psychologists and Code of
Conduct. Washington DC: American Psychological Association.
Chadha, N., & Ratra, A. (2011). Internship Manual. New Delhi: Indira Gandhi National
Open University.
Kukreti, P., & Jiloha, R. C. (2018, February). Psychiatry in Delhi: History and current status.
Indian Journal of Psychiatry, S218-S223.
Mission. (2024). Retrieved April 19, 2024, from Institute of Human Behaviour and Allied
Sciences: https://ihbas.delhi.gov.in/ihbas/mission
Summary Highlights of Annual Report 2016-17. (2017). Retrieved April 19, 2024, from
Institute of Human Behaviour and Allied Sciences:
https://ihbas.delhi.gov.in/sites/default/files/ih/asdcf/aasc/lib/2016.pdf
Vision. (2024). Retrieved April 19, 2024, from Institute of Human Behaviour and Allied
Sciences: https://ihbas.delhi.gov.in/ihbas/vision
World Health Organisation. (1993). The ICD-10 Classification of Mental and Behavioural
Disorders: Clinical Descriptions and Diagnostic Guidelines. Geneva: AITBS
Publishers and Distributors, Delhi.
World Health Organisation. (1997). The ICD 10 International Personality Disorder
Examination. (A. W. Loranger, A. Janca, & N. Sartorius, Eds.) Cambridge:
Cambridge University Press (for WHO). Retrieved April 22, 2024, from
https://iris.who.int/bitstream/handle/10665/41912/9780521041669.pdf




















![Internship Report (MCFTP001)
Page | 37
After this information was gathered, based on which the following genogram was drawn.
Figure 2: Acclimatization Session 1 - Genogram of Kala's Family
After this the interaction continued. The interaction was in Hindi, it has been translated and
reproduced below in English.
T: Since when does she have the problem?
A: This started 1.5 years back. She took medicine for 8-9 months, till then everything was
fine. Then there was a problem, my father expired – because of which she had to leave the
medicine – because she became sedated after taking medicine. Then we felt she became okay,
so we left the medicine.
T: What are the symptoms currently?
A: Talks too much. Breaks things – whatever she sees, she picks and throws. Hitting hands
and legs. Accusing.
T: Accusing people? [Clarification question]
A: Accusing me. That I watch my sister a lot and I give her money. There was a bachelor
living on rent – she used to favour him a lot. Our daughter is young so I asked him to vacate –
she now asks me why I did so.](https://image.slidesharecdn.com/mcftp001internshipreportmsr-250325114943-b3941398/85/IGNOU-Sample-File-for-Internship-MCFTP001-MS-28-320.jpg)
![Internship Report (MCFTP001)
Page | 38
T: Does she see/hear something that others can’t?
A: No. But she was calling the doctor Chacha ji.
T: What happened to her in the first episode?
A: Excessively waving hands and legs. Getting angry without reason. Gesturing in the air.
Her mouth keeps moving by itself. She was sedated. We had to bathe her. She used to do
pray all day.
T: What about the current episode?
A: It’s been going on for 3 days. She touches everyone’s feet, and asks to touch. She takes
water – or anything else – and sprinkles on us.
T: And, between the episodes?
A: She was unable to sleep. She used to get up and sit.
Then the husband started sharing other concerns.
A: Kala puts phone in her ears and keeps talking to her mother who keeps giving her stress.
“You should lock the home” and “Keep your children separate”, and what not! She even calls
the right thing wrong for about 2- 2.5 years. I have been living away since June due to work.
T: What else?
A: She has panic – palpitations (once in 1.5-2 weeks) and also has anxiety. She used to sleep.
Her mother does not trust me as much now.
T: Does she say big things about herself? [Megalomaniac thoughts]
A: “I am Laxmi. Touch my feet.”
T: Any religious behaviours?
A: She prays. Much more during illness.
While this conversation was going on the patient bent and swung her hand.](https://image.slidesharecdn.com/mcftp001internshipreportmsr-250325114943-b3941398/85/IGNOU-Sample-File-for-Internship-MCFTP001-MS-29-320.jpg)
![Internship Report (MCFTP001)
Page | 39
T: [looking at the patient] What are you trying to catch?
P: Parrot.
T: Is it day or night?
P: Day.
[T looks at A who wanted to say something, and indicates him to talk.]
A: Even my daughter has told me you’re not my father now. Kala says her father has passed
away. Her daughter has passed away. She tells our son to marry our daughter.
While the symptoms of the patient were observable, as the husband was living away for the
past few months, he had limited idea about the current set of symptoms.
A session was conducted with the son immediately afterwards – again limited information
was obtained. However, he did mention that there was a fight at home 3-4 days back, after
which the patient became silent and began ruminating.
The son informed that the patient lived in the daughter’s room and spent most time with her.
There was limited interaction with other family members So, it was then decided to interview
the daughter to add more details to the case history. However, the daughter was not in Delhi
at the time.
It was decided by the psychiatrists to admit the patient and start pharmacological treatment
as the diagnoses was clear. That being the case, I did not have further involvement in this
case as there was limited scope of counselling or therapy while the patient was so severely
symptomatic. The family did not seem to be in immediate need of counselling though a
psychoeducation session would have helped.
The symptoms had not receded when I was shifted to the other ward, so I did not get a chance
to interact with the daughter or the other family members in follow up sessions.](https://image.slidesharecdn.com/mcftp001internshipreportmsr-250325114943-b3941398/85/IGNOU-Sample-File-for-Internship-MCFTP001-MS-30-320.jpg)

![Internship Report (MCFTP001)
Page | 41
After this information was obtained from the mother for the genogram (reproduced below).
The only noteworthy new information that emerged was that Sana’s father has alcohol
dependency issue and his elder brother has drug addiction issues.
Figure 4: Acclimatization Session 2 - Genogram of Sana's Family
Observation: While the above conversation was going on, Sana stands up and beats the table
saying random words. She did not respond to the psychiatrist.
T: Has she increased her religious rituals since the illness has started? [Over-Religiosity]
A: Earlier she was more regular. Now the frequency has decreased.
T: Does she have episodes of normality?
A: Yes. Only drowsiness due to medicines is there.
T: Does she always behave like this in her illness?
A: Yes. Though earlier she used to hear voices – of cat crying. [Auditory Hallucinations]
T: Does she take drugs or alcohol?
A: No
Then without any prompting the attendant said that Sana starts crying about her brother.
T: Any problems during the lockdown?](https://image.slidesharecdn.com/mcftp001internshipreportmsr-250325114943-b3941398/85/IGNOU-Sample-File-for-Internship-MCFTP001-MS-32-320.jpg)
![Internship Report (MCFTP001)
Page | 42
A: She used to bathe a lot – while wearing clothes. She used to take-off clothes in front of
anyone. She used to hit – both herself and us. She used to run away from home – very far
away. She used to lie down on the floor, on the footpath.
T: Any megalomaniac thoughts?
A: Yeah. I’m going to marry and go to Mumbai.
T: Asked for new things?
A: Yes. During periods she gets worse.
Once again, she adds information irrelevant to the question, indicating she might have a need
to express herself – and talk to someone regarding the child’s illness or she’s tense about it.
T: When did the current episode start?
A: 4-5 days back. She was also admitted in emergency about 45 days back. She accuses us –
that we don’t give her food and clothes. She considers her younger brother to be enemy, even
her elder sister. Only likes uncle’s wife and children. Loves her elder brother and father. She
abuses. Stubbornly demands food, money and clothes. We have to take medicine from
outside.
T: [looking at P, MSE questions] Is it day or night?
P: There’s light.
T: Who is with you?
P: Asif (younger brother) [Wrong answer, not present]
T: Where do you live?
P: Phone.
A: She salutes everyone. Sings songs. Dances. Talks to herself when alone. Gestures with
fingers. Counts on the inch-tape [used in tailoring]. Gets agitated by her brother and sister.](https://image.slidesharecdn.com/mcftp001internshipreportmsr-250325114943-b3941398/85/IGNOU-Sample-File-for-Internship-MCFTP001-MS-33-320.jpg)
![Internship Report (MCFTP001)
Page | 43
She’s demanding like a young child – “get clothes stitched for me”. When she’s ill, she
hoards garbage. [Again, the mother speaks without question.]
T: Is she able to urinate/defecate normally?
A: She did it in her clothes earlier.
P: [loud and irrelevant] Talk softly.
T: When was her last period?
P: [loud and irrelevant] It’s my papa.
A: 5 days back. On time. For 5-6 days. Normal. She always becomes ill during periods. She’s
very scared of insects since she’s gotten ill. Cats and dogs too. She says “look something’s
walking on my hands and head” [Tactile Hallucinations]
P: [loud and irrelevant] Papa. [Pause] Sunday. Monday.
This session was wrapped up after collecting some more information. Later a session with the
brother was held, where no new facts were revealed.
There were doubts about this being a case of MR, however, considering the current symptoms
it wasn’t possible for an intelligence test to be conducted. Her past report cards were called
for – which showed average performance. VSMS conducted in 2017 was used to ‘diagnose’
moderate MR, however, that is inappropriate use of the test so a proper IQ assessment was
planned after patient gets better – also, it would enable them to get a disability certificate
made.
I had some sessions with the family to counsel them – especially, psychoeducation and
management of the patient. When my internship got over, she was still admitted, undergoing
pharmacological treatment.](https://image.slidesharecdn.com/mcftp001internshipreportmsr-250325114943-b3941398/85/IGNOU-Sample-File-for-Internship-MCFTP001-MS-34-320.jpg)

![Internship Report (MCFTP001)
Page | 45
Based on the observations of the ward staff and during sessions, the father was suspected to
have substance dependence and might possibly have an undiagnosed psychological
condition. The genogram of the patient’s family is given below. The brother is engaged and
supposed to get married soon.
Figure 6: Acclimatization Session 3 - Genogram of Rani's Family
He reported that he was trying to get her married – even to his own friend, so that she could
settle in life. However, she developed this illness. According to him, she had some issues even
before Covid. But, during Covid she stayed locked in single room, so her situation
deteriorated significantly.
Since then, the issues became more and more complex. Gradually, grooming completely
stopped. And, she started calling the police. That is when she was brought to the hospital.
The attendant had been called for a session to get an update on the health condition, but it
turned into a psychoeducation session.
A: Sir, what has happened to Rani? [Looked anxious and flustered]
T: You look anxious Anil. What happened?
A: She keeps saying such bad things. Now, she's saying I murdered my mother for insurance,
and I tried to kill her. She used to say that I hit her and my dad. But now it’s going to the next
level. Why is she lying like this?](https://image.slidesharecdn.com/mcftp001internshipreportmsr-250325114943-b3941398/85/IGNOU-Sample-File-for-Internship-MCFTP001-MS-36-320.jpg)
![Internship Report (MCFTP001)
Page | 46
T: Relax Anil. Have a glass of water. [He was offered a glass of water which he drank.]
After he calmed down.
T: Are you better now?
A: Yes sir. Please tell me why this is happening.
T: It is because of her illness. This is how the patients of this illness often do. What do you
know about her illness?
A: Madam told me she has schizophrenia... Isn't that the same thing in that English movie...
About the mathematician.
T: Which movie? A Beautiful Mind?
A: Yes.
T: Correct, that’s it. What do you know about schizophrenia?
A: That people see things and hear things... That's why we brought her here. She thinks there
are ants roaming about all over her body. And she used to talk to herself. And then she started
fighting with everyone. She says I beat her. She even called the police. We did not have any
option – we had to bring her here. It was too difficult for us! Even we did not want to admit
her to a mental hospital [sense of Stigma], however, we were not left with a choice.
T: Yes. What you’re saying makes sense. And all the things that you have mentioned – they
are normal in her illness.
A: So, all the patients of this illness call the police?
T: Not all. But she has paranoid schizophrenia. And, it isn’t unusual for patients of paranoid
schizophrenia to be scared and take actions to protect themselves – like calling the police.
The counsellor explained in detail, sharing some more examples and working on allaying his
anxieties. The to and fro continued as Anil asked more questions related to the illness.
T: So now, do you have any more questions about it?](https://image.slidesharecdn.com/mcftp001internshipreportmsr-250325114943-b3941398/85/IGNOU-Sample-File-for-Internship-MCFTP001-MS-37-320.jpg)


![Internship Report (MCFTP001)
Page | 49
of compliance to treatment guidelines and to additionally explore any serious inter-personal
issues as the patient had previously reported instances of chaining and beating.
Figure 8: Acclimatization Session 4 - Genogram of Huma's Family
T: Good morning, Huma! How are you now?
P: I have a headache. I get tense when I see fighting. R and A fight. And B hit N on her head
while she was lying down. Even after taking medicine my nerves are hurting.
T: And, sleep?
P: It’s okay.
T: Hunger and thirst?
P: Okay.
Then the patient starts talking about things on her mind, while the counsellor patiently listens
and responds in a way that calms the patient.
P: What should I do here – I don’t understand. If I get involved in a fight, then everyone will
tell me, you are also one of them [mental patient]. It will be better if I die, the load on my
family will reduce. I’m angry with my family – they don’t let me go anywhere – even during
festivals.](https://image.slidesharecdn.com/mcftp001internshipreportmsr-250325114943-b3941398/85/IGNOU-Sample-File-for-Internship-MCFTP001-MS-40-320.jpg)
























![Internship Report (MCFTP001)
Page | 85
Me: Good morning! How are you feeling today?
Peehu: Much better now.
Anya [smiles and nods affirmatively – acknowledging the reported improvement]
Me: Great! Today, we'll look back on what we discussed during counselling and discuss how
to continue improving.
Both: (Nod affirmatively) Sure.
Me: Great! Let's first discuss about the illness and convulsions. Based on our discussions
what do you understand about it?
A discussion happened regarding dissociative disorder and convulsions. The basic concepts
were revisited and focus was on what they could do in case of a convulsion, and what they
could do to prevent it from happening.
Next, we discussed about Problem Solving skills and also the importance of expressive
communication between the parents and children.
Finally, we discussed the future goals and aspirations that were discussed in the previous
session and the patient was reminded of her promise to get back to her studies with full
motivation.
The mother was also reminded that she should get her own treatment done, and if necessary,
get her son and husband evaluated to see if there’s need for treatment or counselling to help
them function better.
During the termination, they were advised to meet the hospital counsellor if required.
Follow up sessions were not necessary, so no advice was given regarding them.
The patient was discharged from the hospital soon after this discussion.](https://image.slidesharecdn.com/mcftp001internshipreportmsr-250325114943-b3941398/85/IGNOU-Sample-File-for-Internship-MCFTP001-MS-75-320.jpg)


















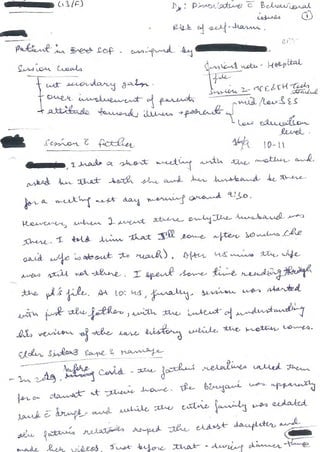
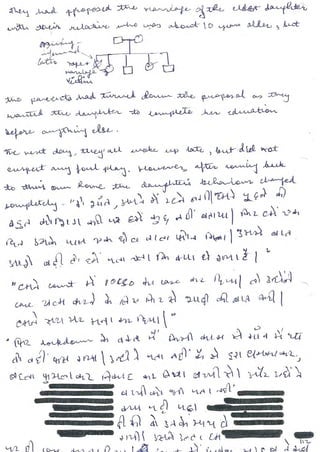












![Internship Report (MCFTP001)
Page | 135
Me: Good afternoon, Pari. How are you feeling now?
Pari: I’m feeling better, thank you.
Ali: I’m fine, too.
Me: Great! Today we will focus on understanding and addressing some of the issues that both
of you are facing due to the illness and the consequent burden on you, Ali. It's important for
all of us to work through these issues together. Are you both comfortable with that?
Both: Yes.
Ali: It is important.
Me: Great. Pari, would you like to share what you feel about the situation?
Pari: [takes a moment to think] Well, it's really hard. Ali has to take so much stress and work
because of my illness. Sometimes, I feel like I'm useless - a burden.
Me: Thank you for sharing, Pari. Ali, how does hearing Pari make you feel?
Ali: [takes a deep breath] It's tough to see her struggle with the illness. But, I'm here for her
no matter what. We''ll get through this together. We have to do it for our children.
Me: That's the spirit, Ali. Pari, how does it feel to hear Ali's support?
Pari: [smiles] It feels good. His support feels good.
Me: It's very important that both of you support each other through this. Now, is there
something in your hearts – about each other – something that makes you angry at the other
person - that you both would like to discuss and clarify today?
Pari: Sometimes I feel he resents me for my illness – and blames me for everything that's
gone wrong.
Ali: (Nods) That is correct – I do get angry at time. It's not because I blame her. I feel
stressed by everything. I feel frustrated sometimes.](https://image.slidesharecdn.com/mcftp001internshipreportmsr-250325114943-b3941398/85/IGNOU-Sample-File-for-Internship-MCFTP001-MS-121-320.jpg)




















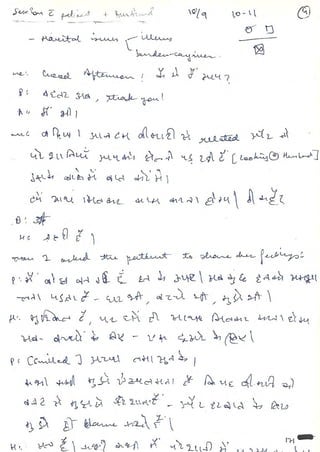


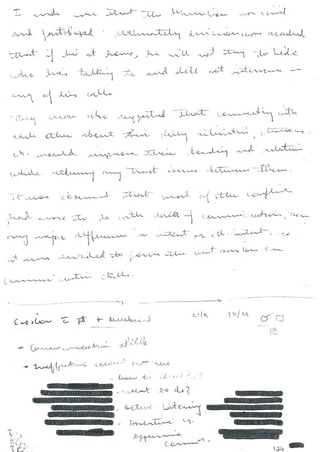




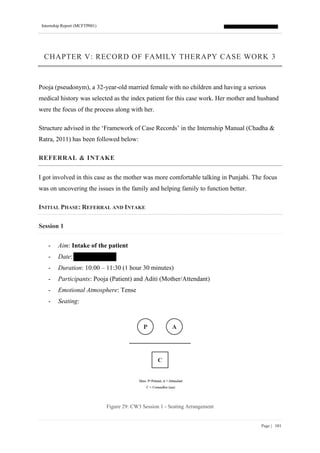




![Internship Report (MCFTP001)
Page | 186
Session 3
- Aim: Identifying Maladaptive Patterns
- Date:
- Duration: 10:00 – 11:00 (1 hour)
- Participants: Pooja (Patient), Aditi (Mother/Attendant) and Hitesh (Husband)
- Emotional Atmosphere: Collaborative
- Seating:
Figure 32: CW3 Session 3 - Seating Arrangement
M: Good morning, everyone! How are you feeling now?
P: I’m okay, thank you.
A: [sighs] It's been a tough week, but things are improving thanks to you.
M: Good to know that things are improving! [paused to emphasise the positive] Today, we
will try to understand how you interact as a family and what challenges you're facing during
interactions. And, if there are any patterns to it.
Are you all comfortable with that?
All: Okay
M: Great! So, first, are there any recurring issues or conflicts that you've noticed – any
patterns of behaviour or communication that are repeated?](https://image.slidesharecdn.com/mcftp001internshipreportmsr-250325114943-b3941398/85/IGNOU-Sample-File-for-Internship-MCFTP001-MS-167-320.jpg)
![Internship Report (MCFTP001)
Page | 187
P: [glancing at her mother and husband before speaking] Hitesh does not have time for me,
he does not even come to meet me and sometimes doesn’t even pick my call.
H: [Sighs] I know, even I feel so. But what can I do – I have to work to pay off…
A: [Interrupting] Is money more important than me?
M: It sounds like there's a communication breakdown here. And, it’s causing tension within
your family. This is a common issue that many families face. [NORMALISATION]
P: [Nodding] Yes. We're stuck, and I don't know how to break free from it.
M: That’s alright. Our goal is to identify these patterns and stop them - and create new, more
positive patterns of interaction. We may need to learn new skills.
All nod in agreement, signalling their understanding.
M: Now, let's explore some more instances where these patterns have emerged in your family
interactions so that we can begin to work towards positive change together.
Session continues with the family members sharing their experiences and insights, identifying
maladaptive patterns and discussing how to change.
M: Our time is up for today, but I want to appreciate you all for your openness and
willingness to explore these issues together. Remember, today we have identified the patterns
– which is the first step towards change.
Session 4
- Aim: Setting Therapy Goals
- Date:
- Duration: 10:00 – 11:00 (1 hour)
- Participants: Pooja (Patient), Aditi (Mother/Attendant) and Hitesh (Husband)
- Emotional Atmosphere: Calm
- Seating:](https://image.slidesharecdn.com/mcftp001internshipreportmsr-250325114943-b3941398/85/IGNOU-Sample-File-for-Internship-MCFTP001-MS-168-320.jpg)






![Internship Report (MCFTP001)
Page | 195
M: "Think of your family as a team on a journey. [USE OF METAPHOR] Sometimes, you
encounter unexpected issues – like delayed trains, lack of food or water, etc. These represent
the problems you're facing. The key is to work together as a team to solve these, and not see
them as your family member’s doing."
I asked them to identify specific challenges they face.
M: "Let's look at some problems you've faced recently. Pooja, perhaps the frustration of not
having Hitesh around as much as you like?"
P: "Yes, exactly. It makes me so sad."
M: "Hitesh, maybe the stress of managing work and family responsibilities?"
H: "Definitely. 'Work Stress' has been a problem."
We discussed externalized problems.
M: " By externalizing these problems, you take a more objective view. It's 'Work Stress' or
'Lack of Intimacy' not someone's fault. How can you, as a team, address these external
forces?"
They collaborate on strategies to overcome the externalized challenges.
P: "Maybe we should plan some time, when he is free."
H: "And setting boundaries with work emails can help."
A: "I can offer to help out more with household work."
M: "Great! Now you're focusing on strategies to solve the problems, not blaming each other."
We followed the same process for some other problems to help them practice well
considering this was a complex process.
M: "Remember, externalizing problems helps you focus on teamwork and problem-solving.
You tackle challenges together, not against each other."](https://image.slidesharecdn.com/mcftp001internshipreportmsr-250325114943-b3941398/85/IGNOU-Sample-File-for-Internship-MCFTP001-MS-176-320.jpg)


































![Internship Report (MCFTP001)
Page | 252
harm done. Even intent of harm could not be conclusively established from the video
‘evidence’ provided by the father. He mentioned there were more videos, which he was asked
to arrange. [The videos were never arranged.]
In addition, the father seemed to be authoritarian and was found to be highly critical of the
patient. The patient was defiant in his behaviour towards father. This was not generalised
towards other authority figures – such as doctors and hospital staff. No one reported any
issues about him. However, several complaints had been received about father’s
argumentative behaviour.
It was decided to proceed and explore the family more through a family interview.
Accordingly, the father was advised to bring the mother and the sister for the next session.
In addition, a three generation Genogram was also created while taking the case history. It
was found that the father also has OCD and is taking ayurvedic medication for the same. No
other issues were reported.
Figure 45: CW4 - Genogram of Pulkit's Family
Session 3
- Aim: Assessment – Family Interview
- Date:
- Duration: 15:00 – 16:00 (1 hour)](https://image.slidesharecdn.com/mcftp001internshipreportmsr-250325114943-b3941398/85/IGNOU-Sample-File-for-Internship-MCFTP001-MS-228-320.jpg)





![Internship Report (MCFTP001)
Page | 259
Session 6
- Aim: Exploring and Improving the Mother-Son and Sister-Brother dyads
- Date:
- Duration: 15:00 – 16:00 (1 hour)
- Participants: Pulkit (Patient), Aditya (Father/Attendant), Mala (Mother) and Sonam
(Sister)
- Emotional Atmosphere: Curious
- Seating:
Figure 49: CW4 Session 6 - Seating Arrangement
Picking up from the last session, they were asked if they were ready to put in the effort to
improve their family’s situation. They expressed their eagerness to improve the situation and
stated they were willing to do anything to make it happen.
Me: Good! So today we will discuss Pulkit’s relation with Mala and Sonam.
So, I proceeded with further investigating the intra-dyad dynamics of the mother and sister
with the patient, to understand what was driving the issues and to improve them.
Me: First, let’s discuss about the relation between Pulkit and Sonam. Pulkit what happened
that made you attack her? [NOTE THE AVOIDANCE OF WHY]
P: She says bad things about me and mocks me – calls me useless, failure, loser...
S: I just do it because I get irritated with what is going on. I don’t mean to hurt him.](https://image.slidesharecdn.com/mcftp001internshipreportmsr-250325114943-b3941398/85/IGNOU-Sample-File-for-Internship-MCFTP001-MS-235-320.jpg)

![Internship Report (MCFTP001)
Page | 261
Perhaps, this session itself could be enough for it.
Session 7
- Aim: Exploring and Improving the Mother-Daughter and Husband-Son Dyads
- Date:
- Duration: 12:00 – 13:00 (1 hour)
- Participants: Pulkit (Patient), Aditya (Father/Attendant), Mala (Mother) and Sonam
(Sister)
- Emotional Atmosphere: Solution-focused
- Seating:
Figure 50: CW4 Session 7 - Seating Arrangement
I welcomed them and congratulated on the progress so far.
Me: Today, we’ll discuss about Aditya and Mala’s relation and Mala and Sonam’s relation.
Let’s start with Mala and Sonam. Sonam what would you like to say about your relation with
your mother?
S: She is very nice and caring. I have only one issue that whenever something happens, she
sides with papa. Like, in the case of Scooty.
M: [nodded and smiled embarrassedly]
The mother was counselled to be more rational and play the role of a neutral moderator
when conflict like situations happen at home. I asked her:
Me: When you were a teacher and conflict happened in class, did you side with one person?](https://image.slidesharecdn.com/mcftp001internshipreportmsr-250325114943-b3941398/85/IGNOU-Sample-File-for-Internship-MCFTP001-MS-237-320.jpg)







![Internship Report (MCFTP001)
Page | 269
Figure 55: CW4 Session 12 - Seating Arrangement
Considering the family was at a breaking point at the beginning of the sessions, the distance
they had covered in the short span of time was phenomenal. It was important to celebrate this
victory so that they have a sense of achievement. This shared success would contribute
further to their reintegration and further improvement in their family dynamics.
Me: Today, let's reflect on our progress so far. When we had the first session, the
communication was strained, there was a lot of conflict and there seemed to be no end to the
problems.
Followed by highlighting their specific improvements in communication, problem-solving,
and emotional expression – congratulating them on their successes.
P: I'm very happy to see how far we've come. [Others nod in agreement.]
A: It's been a challenging journey, but I'm proud of how much we've grown as a family.
Me: These changes took effort from everyone – well done! Now, let's reevaluate the situation
and compare it to when the sessions started.
Family remembers the negative aspects and realises the positive changes achieved. Overall,
as desired, the session ended with the family feeling positive about their achievements during
the sessions so far. Thus, they were now ready for termination.
Session 13
- Aim: Termination
- Date:](https://image.slidesharecdn.com/mcftp001internshipreportmsr-250325114943-b3941398/85/IGNOU-Sample-File-for-Internship-MCFTP001-MS-245-320.jpg)















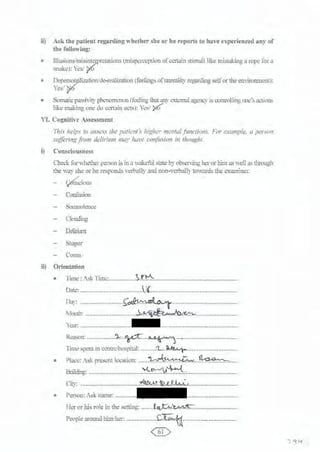




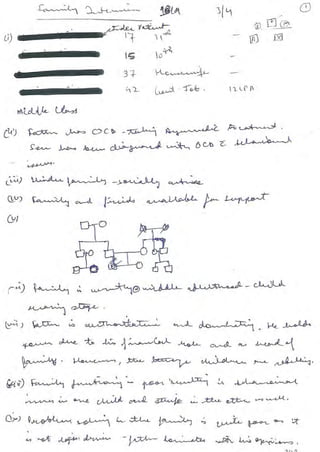
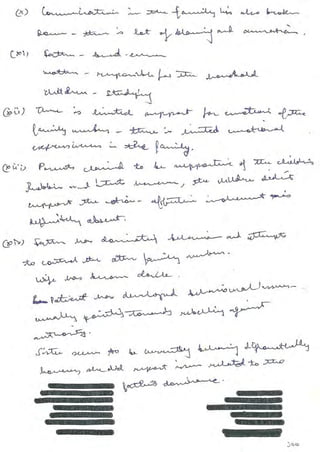
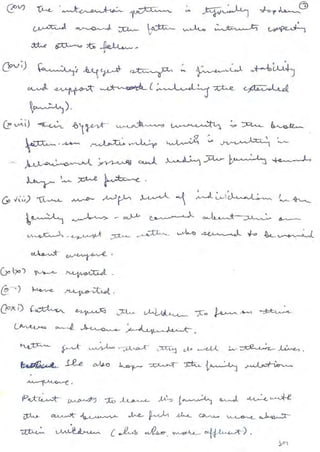




























































































![Polymer [ बहुलक ] Chemistry Notes PDF - Irfanullah Mehar - JJ Sir Chemistry.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/polymerchemistrynotespdf-irfanullahmehar-jjsirchemistry-260210172118-3f9b37f7-thumbnail.jpg?width=640&height=640&fit=bounds)

