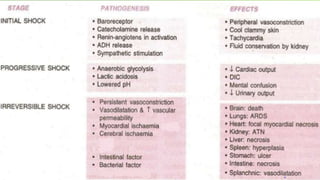
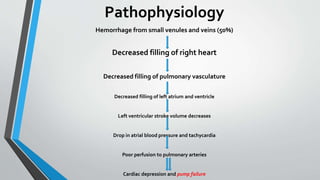
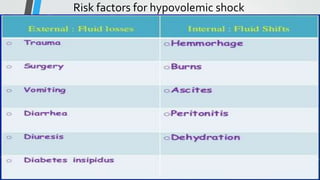
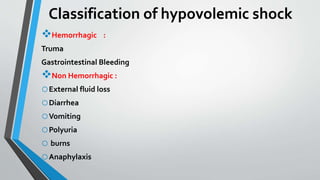
Shock is defined as inadequate delivery of oxygen and nutrients to tissues and cells. It occurs in 2% of hospitalized patients and mortality depends on the underlying cause. Pathophysiology involves reduced blood flow from decreased circulating volume or cardiac dysfunction. Stages include initial compensated shock progressing to decompensated irreversible shock. Types are hypovolemic, cardiogenic, distributive, obstructive, and septic shock. General signs are hypotension, tachycardia, coldness, rapid breathing, and organ dysfunction. Hypovolemic shock results from blood or fluid loss which decreases venous return and cardiac output. Risk factors include trauma, bleeding, burns, and dehydration. Treatment focuses on fluid res
![Cont.…
Resuscitation
Immediate control of bleeding (rest , pressure Peking and surgical
methods)]
Infusion of fluid is the fundamental treatment
Crystalloids fluid
Colloids fluid (after crystalloid)
Drugs :
1.sedatives
2.chronotropic agent
3.inotropic agent](https://image.slidesharecdn.com/hypovolemicshock-201208185153/85/Hypovolemic-shock-21-320.jpg)