
Downloaded 23 times









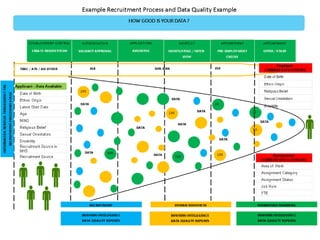


The document details an event hosted on October 1, 2015, at the Royal Marsden Education and Conference Centre, focusing on data quality and standards in health and social care. Presentations covered the importance of data quality for effective decision-making, recent developments in NHS data standards, and strategies for improving the Electronic Staff Record (ESR) system. Key objectives included fostering collaborative working, highlighting available tools and guidance, and addressing data quality issues through interactive discussions and feedback from attendees.









































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)













