Download to read offline



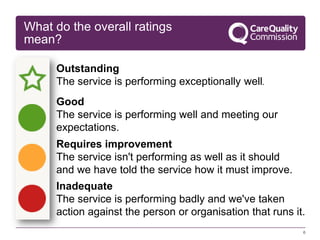

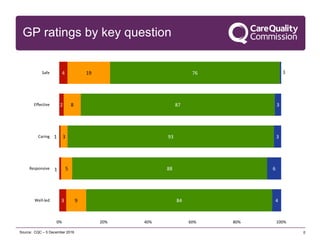

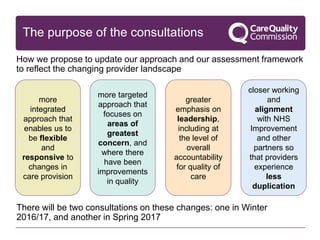
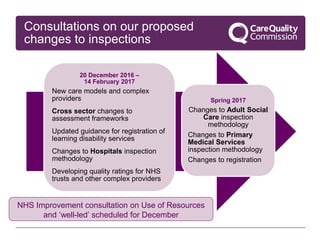







The document provides an overview of the Care Quality Commission (CQC) and its role in regulating health and social care services in England. Some key points: - CQC registers providers, monitors and inspects services to assess safety, effectiveness, caring, responsiveness and leadership. It publishes ratings and takes action on poor care. - Most GP practices provide good quality care, with 87% rated good or outstanding. Strong leadership and governance are important for delivering high quality care. - CQC is moving to a more targeted and responsive approach focused on greatest risks. It will work more closely with other organizations to reduce duplication for providers. - Upcoming consultations will seek feedback on proposed changes to inspection



















![New clinical quality measure reporting in Practice Fusion [slides]](https://cdn.slidesharecdn.com/ss_thumbnails/junecqmwebinarslideshare-140611132004-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)



































































