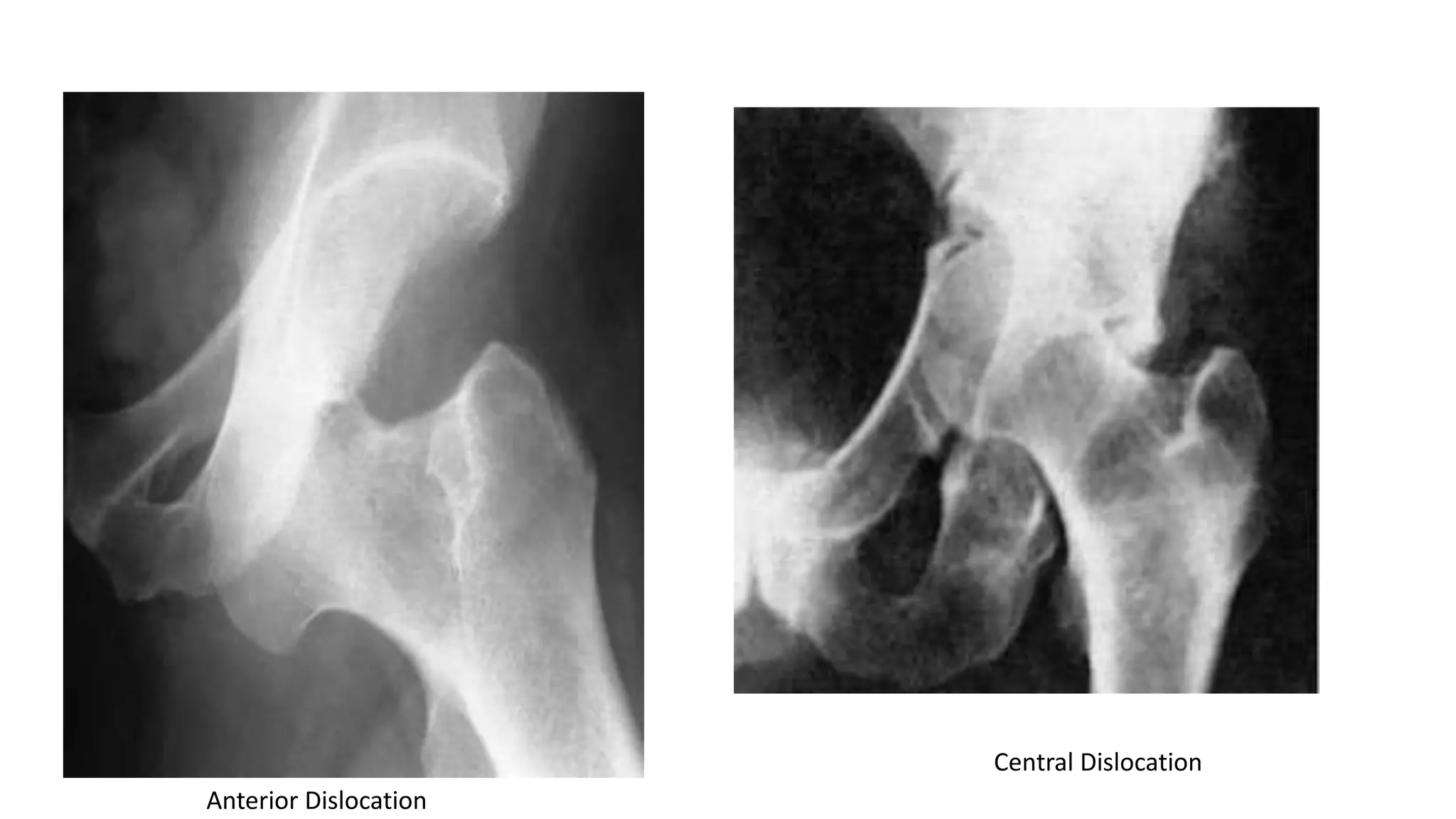
Hip dislocations are classified by the direction of femoral head displacement as posterior, anterior, or central. Posterior dislocations are the most common, often resulting from high-energy trauma like motor vehicle accidents. They require closed reduction under anesthesia which may be difficult due to bone fractures. Anterior dislocations are rare but can occur from abduction and external rotation of the hip. Central dislocations actually involve an acetabular fracture displacing the femoral head medially. All hip dislocations require prompt reduction to prevent long-term complications like avascular necrosis or osteoarthritis.