Diagnosis of Pregnancy&
Antenatal Care
5th
year lecture
Dr. Vanilla Banda
BSc. HB, MBChB, MMed (OBGY)-[UNZA]
University Teaching Hospitals (UTHs)- Women & Newborn
Hospital
Date: 23-08-2022
03/10/25 1
2.
Outline
• Diagnosis ofpregnancy
• Principles of diagnosis of pregnancy
• Symptoms of pregnancy
• Signs of pregnancy
• Investigations
• Antenatal care
• Components of individual birth plan
03/10/25 2
Principles of dxof pregnancy
• Most women ,dx is based on Hx of
amenorrhea & positive pregnancy test.
• Women with irregular menses, dx is complex.
• Other symptoms of pregnancy may alert
clinician on possibility of pregnancy.
03/10/25 4
5.
Symptoms of pregnancy
•Amenorrhoea; pregnancy may occur during
period of lactation amenorrhoea.
• Slight bleeding in early pregnancy may be
considered normal menses.
• Slight bleeding may occur at time of
implantation.
• Morning sickness: nausea, vomiting confined
to morning
03/10/25 5
6.
Symptoms cont.
• Cessationof menstruation
• Easy fatigueability & tendency to sleep.
• Emotional changes e.g. change of appetite
• ↑ frequency of micturition.
• Enlargement of breasts & sensation of heaviness.
• Abdominal enlargement
• Quickening-1st
perception of fetal movements by
woman.
• PG (18-20), MP (16-18 weeks).
03/10/25 6
7.
Signs of Pregnancy
•Chloasma gravidarum
• Butterfly face
• Pigmentation
• Breast signs– ↑pigmentation of nipple &
areola.
• Appearance of Montgomery tubercle in the
areola, dilated sebaceous glands.
03/10/25 7
8.
Abdominal signs
• Inspection- Abdominal stria, linea nigra, fetal
movements as early as 20 weeks.
• Determination of the HOF- uterine size
palpable by 12 weeks GA.
• Auscultation- FHS can be done as early as 20-
24 by pinard stethoscope.
03/10/25 8
9.
Investigations
• Detection ofHCG in urine or serum confirms
pregnancy.
• Classically, urinary pregnancy test becomes +ve 7-10
days after 1st
missed period.
• By time mom has missed her 1st
menstrual period,
HCG levels are ~ 100 iu/L.
• Serum pregnancy test classically becomes +ve 5-7
days before 1st
missed period.
03/10/25 9
10.
Investigations cont.
• Aquantitative serum HCG assay level of 5iu/L
will usually denote a pregnancy.
• With a normal intrauterine pregnancy, HCG
level will double approx. every 36- 48 hrs.
• Ultrasound will confirm pregnancy.
03/10/25 10
• Definition: Refersto heath care provided to
pregnant woman throughout pregnancy until
beginning of labour.
• Overall purpose is to optimize outcome of
pregnancy for mom, her baby & rest of family
• Comprises: Careful history taking and
examination and advice to the pregnant
woman
Antenatal care
03/10/25 12
13.
Goals
• Ensure thatthe mother is health.
• Ensure delivery of a health infant.
• Anticipate problem.
• Diagnose problems early.
03/10/25 13
14.
Objectives
• Early detection& if possible, prevention of
complications of pregnancy.
• Educate women on danger & emergency signs &
symptoms.
• Prepare woman & her family for childbirth.
• Give education & counselling on family planning.
03/10/25 14
15.
Criteria
•The criterion ofnormal pregnancy care;
delivery of a single baby in good condition at
term (between 37-41 weeks) with a fetal weight
of 2.5 – 3.5kg & without maternal complication.
03/10/25 15
16.
Schedule of antenatalcare
• Medical check up every 4 weeks up to 28
weeks gestation.
• Every 2 weeks until 36 weeks of gestation.
• Every week until delivery but not beyond 41
weeks.
• An average 8-10 antenatal visits .
• More frequent visits may be required if
complications arise.
03/10/25 16
17.
First Visit (BookingVisit)
• Should be preferably done before the second missed
period or after confirmation of pregnancy. WHO
(before 12weeks)
• Take a full history, examination & investigation.
• Objectives
– To assess the health status of the mother
– To assess the fetal viability + gestation age and to obtain
baseline investigations
– To organize continued care and risk assessment
03/10/25 17
18.
First Visit: History
•Accurate dating of gestational age
• Any symptoms – minor or major complaints
• Fetal movement perception
• ANC details – investigations & interventions
• Past obstetric history – Details of any obstetric
complications in previous pregnancies
03/10/25 18
19.
First Visit: History(Cont’d)
• Family history
– Any familial medical conditions
– Family history of congenital anomalies; multifetal
gestations and hypertensive disorders of
pregnancy
• Past medical history
– History of medical illnesses
• Social History
– Smoking, alcohol intake & habitual drugs use
03/10/25 19
20.
Menstrual history
• Askabout- last menstrual period (LMP).
• Regularity and frequency of menstrual cycle.
• Contraception method used.
• Calculate expected date of delivery (EDD) as 1st
day
of LMP -3 months+7 days & change the year.
03/10/25 20
21.
Obstetric History
• Gravidity?Parity? Abortion & living children.
• Weight of infant at birth and duration of
gestation.
• Mode of delivery .
• Maternal or infant complications.
03/10/25 21
22.
Medical and surgicalHistory
• Chronic conditions: as DM, HTN & renal
disease, cardiac disease.
• Previous operation: cesarean section , genital
repair & cervical cerclage .
• Accidents involving injury to the bony pelvis.
03/10/25 22
Emergency symptoms (Redflags)
• Vaginal bleeding
• Severe abdominal, epigastric or pelvic pain
• Severe headache with visual disturbance
• Persistent vomiting
• Unconsciousness/ convulsions
• Difficulty in breathing
• Fever, chills
• Absent fetal movements.
03/10/25 24
25.
First visit: Examination
•Vital signs & anthropometry (weight & height)
• Detailed physical exam from head to toe for medical
or surgical illnesses.
• Check for nutritional status of the woman.
• Check for for pallor or anemia (Palmar &
conjunctival) .
• Check for oedema .
• Urine for protein & sugar.
03/10/25 25
26.
Examination Cont.
• Abdominalexam
– Fundal height by symphysis-fundal height measurement by the tape method
– Fetal heart auscultation after 10th week by doppler or 20th week by fetal heart stethoscope
– Fetal presentation after the 28th week but malpresentations abnormal after the 34th week
• Symphysis fundal height :
LMP plus 280 days
Add 7 days , subtract 3 months
MacDonald’s Rule (cm= weeks).
03/10/25 26
27.
Investigations
• Get baselineon the first or following the first
visit.
- FBC/Hb, ABO and Rhesus, RBS,RVT,
- VDRL or RPR to screen for syphilis,
- HBsAg test.
• Imaging: Booking U/S for viability +GA.
03/10/25 27
28.
Supplementation
• Folic acid,Iron (ferrous sulphate or gluconate)
• Deworming drugs e.g. mebendazole
• Anti- malarial e.g. fansidar 1st
dose to be given at 13
weeks.
• Nutritional supplement optional
• Commencement of ART if Reactive.
• Tetanus toxoid
03/10/25 28
29.
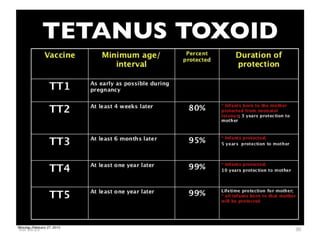
Tetanus Toxoid
• 0.5mL of tetanus toxoid IM.
• 5 doses give life long
protection.
• No maximum interval
between doses.
• TT doses received in school
should be included in the
required 5 doses.
03/10/25 29
• Routine activitiesin ANC clinic: BP, weight, Urinalysis,
nutritional advise, health education messages on
pregnancy, delivery danger signs & hygiene.
• Assessment of fetal & maternal wellbeing.
• At each visit birth preparedness should be emphasized.
• Danger signs in pregnancy & importance of institutional
delivery by skilled attendant.
Routine antenatal care
03/10/25 31
32.
Components of IndividualBirth Plan
• Does your client know when her baby is due?
• Has she identified a skilled birth attendant?
• Has she identified a health facility to deliver from?
• Can she list danger signs in pregnancy and delivery?
• Has she identified a decision maker in case of an
emergency?
03/10/25 32
33.
Components of IndividualBirth Plan (Cont’d)
• Does she know where/how to get money in case of
an emergency?
• Does she have a transport plan in case of an
emergency?
• Does she have a support person in case of an
emergency?
• Has she collected the birth supplies for the birth?
03/10/25 33
![Diagnosis of Pregnancy &
Antenatal Care
5th
year lecture
Dr. Vanilla Banda
BSc. HB, MBChB, MMed (OBGY)-[UNZA]
University Teaching Hospitals (UTHs)- Women & Newborn
Hospital
Date: 23-08-2022
03/10/25 1](https://image.slidesharecdn.com/antenatalcare2022-250310013011-7c836672/85/Antenatal-care-2022-ppt-1-320.jpg)
![Diagnosis of Pregnancy &
Antenatal Care
5th
year lecture
Dr. Vanilla Banda
BSc. HB, MBChB, MMed (OBGY)-[UNZA]
University Teaching Hospitals (UTHs)- Women & Newborn
Hospital
Date: 23-08-2022
03/10/25 1](https://image.slidesharecdn.com/antenatalcare2022-250310013011-7c836672/75/Antenatal-care-2022-ppt-1-2048.jpg)











![Prenatal[2]](https://cdn.slidesharecdn.com/ss_thumbnails/prenatal2-120201220630-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Prenatal[2]](https://cdn.slidesharecdn.com/ss_thumbnails/prenatal2-120201201254-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Prenatal[3]](https://cdn.slidesharecdn.com/ss_thumbnails/prenatal3-120201200622-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)









![Prenatal[3]](https://cdn.slidesharecdn.com/ss_thumbnails/prenatal3-120201220429-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
























