Downloaded 223 times



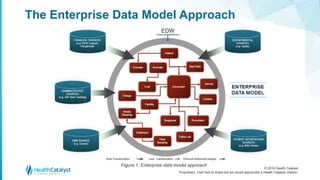















The document outlines various healthcare data warehouse modeling approaches, particularly contrasting the traditional enterprise data model and independent data mart models with Health Catalyst's late-binding approach. Traditional models often lead to delayed value and lack adaptability, whereas the late-binding method allows for flexible data integration and timely binding to address changing business needs. The late-binding approach provides a more practical framework for building a healthcare data warehouse that accommodates rapid shifts in healthcare analytics requirements.