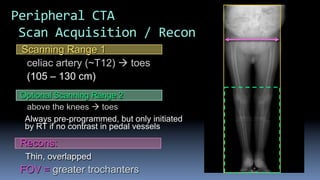
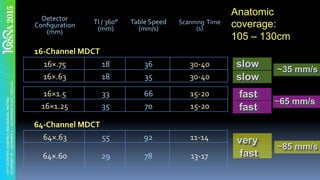
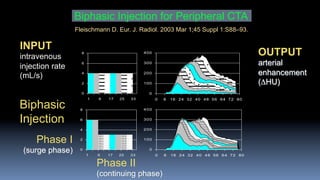
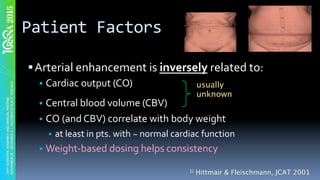
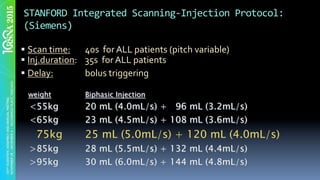
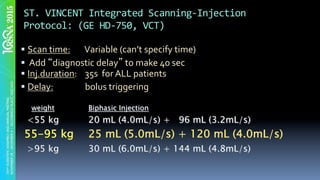
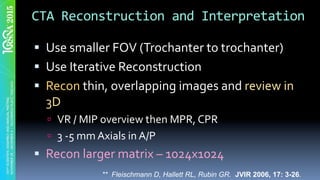
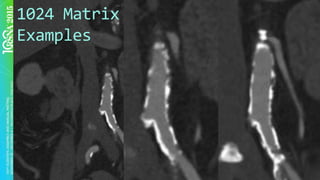
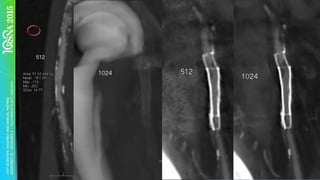
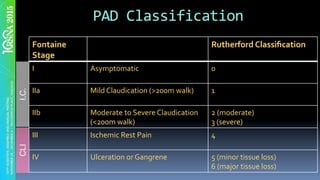
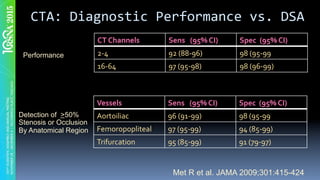
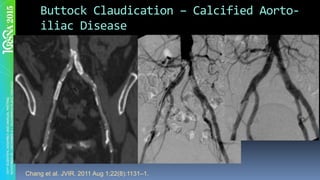
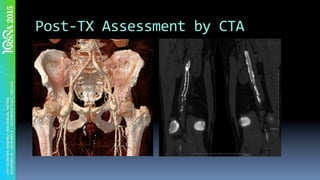
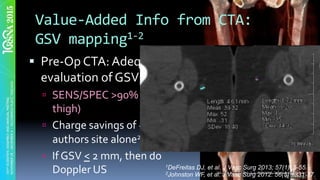
The document discusses the use of Computed Tomography Angiography (CTA) for evaluating peripheral artery disease (PAD), outlining acquisition techniques, clinical efficacy, and cost-effectiveness. It emphasizes the importance of proper contrast administration and scanning protocols, as well as the diagnostic performance of CTA compared to traditional Digital Subtraction Angiography (DSA). The conclusions highlight CTA's accuracy and its integrated scanning-injection protocols for enhanced consistency in patient assessments.